How Sleep Affects Work Performance: What the Evidence Shows
Short sleep is one of the largest unaddressed productivity drains in modern work — and the people losing the most cognitive performance are usually the least aware of it. Here is what the published evidence actually shows, from the Van Dongen dose-response study to RAND's $411 billion estimate.
How sleep affects work performance is no longer a question of opinion. Roughly 30% of US adults sleep fewer than seven hours on a typical night (CDC National Center for Health Statistics, 2024), and three decades of controlled laboratory work, occupational field studies, and large economic analyses now converge on the same point: a chronic shortfall of one or two hours per night accumulates into a measurable cognitive deficit that workers carry into meetings, decisions, deliverables, and the drive home.
The mechanism is not what most people picture. The dangerous form of sleep loss is not the occasional all-nighter — it is the steady erosion of one or two hours, night after night, that workers stop noticing within a few days. This guide walks through the evidence in six parts: the cognitive mechanism, the awareness gap that makes the problem invisible, the alcohol-equivalence framing that anchors the size of the deficit, the workplace and traffic safety record, the GDP-scale economic cost, and what the published interventions actually show.
How Sleep Affects Work Performance at the Cognitive Level
Three decades of laboratory work have converged on a finding that contradicts office intuition: chronic short sleep is worse for cognitive performance than an occasional all-nighter. Van Dongen, Maislin, Mullington & Dinges (2003, Sleep 26:117–126) randomized subjects to four hours, six hours, or eight hours of time in bed for fourteen consecutive nights, with a parallel three-night total sleep deprivation arm, and measured vigilant attention, working memory, and cognitive throughput throughout. The result, in the paper's own abstract wording: "chronic restriction of sleep to 6 h or less per night produced cognitive performance deficits equivalent to up to 2 nights of total sleep deprivation." The deficit accumulated linearly across the two weeks; there was no plateau.
Lim & Dinges (2010, Psychological Bulletin 136:375–389) pooled 70 studies covering 147 cognitive tests and confirmed that the single most sleep-sensitive measure is vigilant attention — the simple, sustained-attention reaction-time tasks captured by the Psychomotor Vigilance Test (PVT). Working memory, processing speed, short-term memory, and reasoning are all impaired by short sleep, but lapses in vigilant attention show the largest and most consistent effect sizes. The PVT is now the standard outcome measure in fatigue research precisely because of this sensitivity.
The earlier meta-analysis from Pilcher & Huffcutt (1996, Sleep 19:318–326), based on 143 study coefficients across roughly 1,932 subjects, established the ordering of impairment that still holds today: mood is more affected than cognitive performance, which is more affected than motor performance. The same paper isolated a finding that matters most for office work: "partial sleep deprivation has a more profound effect on functioning than either long-term or short-term sleep deprivation." The slow, daily erosion of one or two hours is the costly form. The dramatic single all-nighter is, on average, less destructive than two weeks of going to bed an hour late.
Why You Don't Feel the Cost
The secondary finding from Van Dongen 2003 is arguably more consequential than the primary one. As the fourteen-day sleep restriction progressed, the cognitive performance of the four-hour and six-hour groups continued to decline — but their subjective sleepiness ratings plateaued after the first few days. They stopped feeling worse even though they kept getting worse. In the paper's exact wording, subjects "were largely unaware of these increasing cognitive deficits."
This dissociation between perceived and actual impairment matters in the workplace. The colleague who says "I'm fine, I only got six hours" is making a statement about their feeling, not about their measurable performance. The two are not the same metric. Sleep researchers have likened the gap to the well-documented one for alcohol: intoxicated drivers reliably underestimate their impairment, and so do sleep-restricted workers. Self-report is unreliable in both directions — overconfident at moderate impairment, and offering no internal warning before performance has already degraded.
The practical implication is that a workplace cannot rely on people noticing when they are too tired to make a high-stakes decision. By the time someone feels too tired to safely sign off on a deliverable or drive home, they are typically well past the point of measurable impairment.
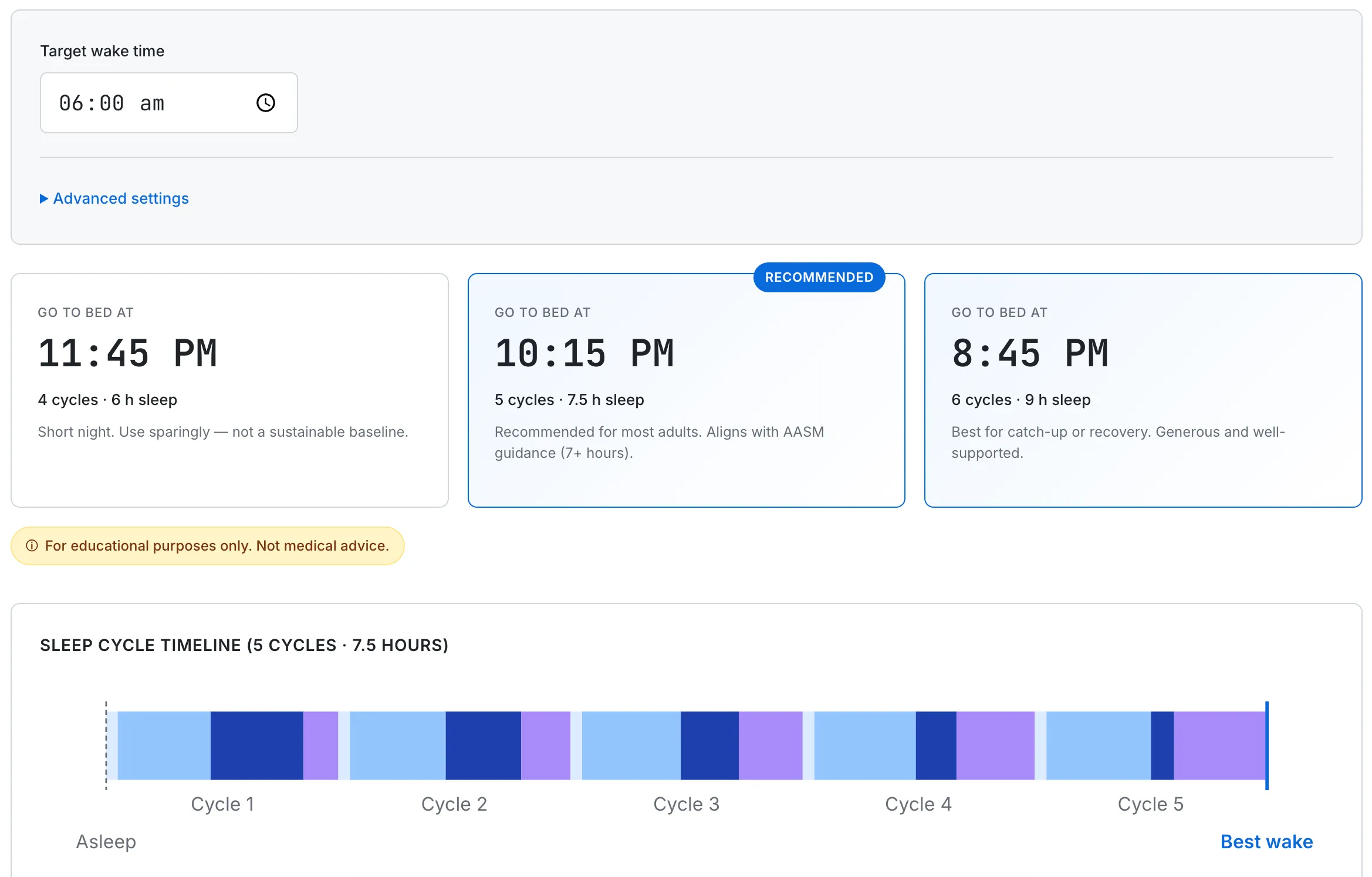
SudoTool's Sleep Cycle Calculator — work backward from a fixed wake time to find a bedtime that hits the AASM seven-hour minimum.
Sleep Deprivation Looks Like Alcohol Intoxication
Two independent studies have measured the impairment of sustained wakefulness against the impairment of measured alcohol intoxication, using the same psychomotor tests in the same subjects. The framing is striking enough that it has become the single most-quoted comparison in occupational sleep research.
Dawson & Reid (1997, Nature 388:235), in a one-page Nature brief communication, reported that cognitive psychomotor performance after roughly 17 hours of sustained wakefulness has been observed as comparable to a blood alcohol concentration of approximately 0.05%, and that performance after about 24 hours awake approached the equivalent of approximately 0.10% — above the legal driving limit in most jurisdictions.
Williamson & Feyer (2000, Occupational and Environmental Medicine 57:649–655) replicated and extended the finding in a more naturalistic occupational sample — 39 subjects, 30 of them transport-industry employees and 9 from the army, studied over a 28-hour sleep deprivation protocol with parallel alcohol doses up to BAC 0.10%. In the paper's own wording: "After 17–19 hours without sleep, … response speeds were up to 50% slower for some tests and accuracy measures were significantly poorer than at this level of alcohol" (where "this level" is BAC 0.05%). With longer wakefulness, performance reached the equivalent of the maximum alcohol dose given, BAC 0.10%.
The arithmetic is uncomfortable. A worker who wakes at 6:00 AM and is still on the job at 11:00 PM has crossed the 17-hour threshold. By the time they drive home, by the time they answer the last critical chat message, by the time they sign off a deliverable, their measurable cognitive performance is no better than someone with a legally consequential amount of alcohol in their bloodstream. Most workplaces would not tolerate the second; many tolerate the first as ordinary professionalism.
Errors at Work and Behind the Wheel
Two well-controlled studies anchor the workplace-error evidence at the top of medicine, and one recent national analysis anchors the transport side. Landrigan, Rothschild, Cronin and colleagues (2004, New England Journal of Medicine 351:1838–1848) randomly assigned hospital interns in two intensive care units to a traditional schedule with 24-hour-plus shifts every third night, or to an intervention schedule with no extended shifts and reduced weekly hours. The intervention was, in effect, more sleep.
The results, from the paper's own abstract: "interns made 35.9 percent more serious medical errors during the traditional schedule than during the intervention schedule (136.0 vs. 100.1 per 1,000 patient-days, P<0.001)" and "5.6 times as many serious diagnostic errors during the traditional schedule … (18.6 vs. 3.3 per 1,000 patient-days, P<0.001)." The same NEJM issue published Lockley et al.'s companion paper showing significantly more attentional failures on the extended schedule. The patients of better-rested interns received measurably safer care.
Outside the hospital, the largest single category of measurable harm from sleep loss is driving. The AAA Foundation for Traffic Safety 2024 analysis ("Drowsy Driving in Fatal Crashes, United States, 2017–2021") used a statistical model trained on National Highway Traffic Safety Administration in-depth crash investigations to impute drowsy-driver involvement in fatal crashes nationwide. An estimated 17.6% of all fatal crashes in 2017–2021 involved a drowsy driver — 29,834 fatalities over the five-year period. That figure is roughly ten times higher than traditional police-reported drowsy-driving estimates, because drowsiness is rarely identifiable at the scene after the fact. The earlier alcohol-equivalence math is the mechanism: a late-night drive home crosses the 17-hour-awake threshold for many workers without anyone in the car recognizing it as the equivalent of driving impaired.
The Aggregate Economic Cost
The aggregate workplace cost of sleep loss is large enough to be visible at the GDP level. RAND Europe's Why Sleep Matters cross-country analysis (Hafner, Stepanek, Taylor, Troxel & van Stolk, 2017, RAND Health Quarterly 6(4):11) modeled the economic burden of insufficient sleep across five OECD countries using mortality, morbidity, productivity, and absenteeism inputs. The US-specific numbers are blunt:
- Up to $411 billion per year in economic losses from insufficient sleep — 2.28% of US GDP under the report's most optimistic scenario.
- Approximately 1.2 million working days lost annually in the US to sleep-related productivity decrements.
- People sleeping less than six hours per night carry a 13% higher mortality risk than those sleeping between seven and nine hours.
- If those currently sleeping under six hours moved into the six-to-seven-hour band, RAND estimated approximately $226.4 billion would be added to the US economy.
RAND's $411 billion is the upper bound of their model. Even the lower bound is a number that dwarfs most line items on a corporate productivity profit-and-loss statement — and unlike most line items, sleep loss is not a fixed-overhead cost that someone has already chosen to pay. It is a leak. Our true cost of meetings post covers the analogous math for synchronous time; sleep loss compounds with the meeting baseline rather than substituting for it.
What the Evidence Says Actually Helps
The evidence base supports a short list of interventions that have measurable effect on cognitive performance at work:
1. Hit seven hours on a regular basis. The 2015 American Academy of Sleep Medicine and Sleep Research Society joint consensus statement (Watson et al., Journal of Clinical Sleep Medicine 11(6):591–592) was built from a twelve-month review of 5,314 scientific articles across nine health domains by a fifteen-member expert panel using a modified RAND Appropriateness Method. The recommendation, verbatim: "Adults should sleep 7 or more hours per night on a regular basis to promote optimal health." The National Sleep Foundation's 2015 recommendations (Hirshkowitz et al., Sleep Health 1(1):40–43) give a 7–9 hour range for young adults and adults, 7–8 hours for older adults, and 8–10 hours for teenagers. Numbers below those ranges trade short-term feelings of being okay for long-term measurable performance loss — see our hours of sleep by age guide for the full breakdown.
2. Consistency beats catch-up. Van Dongen's cumulative-excess-wakefulness model implies that the deficit accumulates daily; weekend recovery sleep produces only partial recovery, and not on the schedule a typical workweek requires. The practical translation is a stable wake time anchored regardless of bedtime, then working backward to a bedtime that hits the seven-hour minimum. Our is six hours of sleep enough post covers what the recovery research actually shows about chronic six-hour nights.
3. The NASA short nap. Rosekind, Graeber, Dinges and colleagues (1995, NASA Technical Memorandum 108839) studied planned 40-minute cockpit rest periods in long-haul commercial pilots; actual mean sleep within those periods was about 26 minutes after roughly 6 minutes of sleep latency. The pilots in the rest condition had roughly 30% fewer reaction-time lapses on subsequent in-flight psychomotor vigilance tests than the no-rest control group, and in the critical 90 minutes before top of descent the no-rest group averaged 6.37 EEG/EOG microevents indicative of reduced physiological alertness versus 2.90 in the rest group — roughly a 54% reduction. Keeping the nap under 30 minutes is the operative detail: it stays in light sleep and avoids the post-nap "sleep inertia" that longer naps produce.
4. Stop caffeine well before bed. Caffeine has a half-life of roughly five to six hours in most adults, so an afternoon coffee is still measurably in your system at midnight. The specific cutoff that protects sleep onset and sleep architecture is covered in our caffeine and sleep cutoff post — the practical bottom line is that the meaningful intervention is timing, not switching to decaf at 9 PM.
5. Know when to escalate. Chronic insomnia, suspected sleep apnea, and shift-work disorder are clinical conditions, not productivity problems that can be fixed by better calendar management. If you have consistently hit seven-plus hours for several weeks and still feel non-restored, our why am I tired after eight hours of sleep post covers the differential and the threshold for a clinical evaluation.
The single largest leverage on cognitive performance at work is not a new tool, a new framework, or a new app. It is the unglamorous intervention of getting one more hour of sleep on a regular basis. The math is in RAND's $411 billion estimate, in Van Dongen's six-hour cohort, in Williamson and Feyer's seventeen-hour reaction-time data, in Landrigan's 35.9% serious-error gap. The intervention works because the deficit is real, measured, and largely unfelt — which makes the deficit invisible to the person who has it, and the recovery just as invisible to the person who finds it. The published evidence is the only way to see either one. For the focus side of the equation, our deep work for software developers guide covers what sustained concentration actually requires once the sleep precondition is in place, and the multitasking myth covers the cognitive switching cost that short sleep amplifies.
This is a general productivity and cognitive-science guide, not personalized medical, occupational, or workplace advice. Chronic insomnia, suspected sleep apnea, shift-work disorder, and other clinical sleep conditions can produce symptoms that overlap with simple short-sleep effects but require a different evaluation; if symptoms persist after consistent seven-plus hour nights, consult a licensed clinician. Mortality, accident, and economic statistics quoted here are population-level estimates and do not predict individual outcomes.
- Van Dongen, H.P.A., Maislin, G., Mullington, J.M. & Dinges, D.F. (2003). The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep 26(2):117–126. PubMed · PDF (Penn UEP).
- Lim, J. & Dinges, D.F. (2010). A meta-analysis of the impact of short-term sleep deprivation on cognitive variables. Psychological Bulletin 136(3):375–389. PubMed.
- Pilcher, J.J. & Huffcutt, A.I. (1996). Effects of sleep deprivation on performance: a meta-analysis. Sleep 19(4):318–326. PubMed.
- Dawson, D. & Reid, K. (1997). Fatigue, alcohol and performance impairment. Nature 388(6639):235. Nature.
- Williamson, A.M. & Feyer, A-M. (2000). Moderate sleep deprivation produces impairments in cognitive and motor performance equivalent to legally prescribed levels of alcohol intoxication. Occupational and Environmental Medicine 57(10):649–655. PMC full text.
- Landrigan, C.P., Rothschild, J.M., Cronin, J.W., et al. (2004). Effect of reducing interns' work hours on serious medical errors in intensive care units. New England Journal of Medicine 351(18):1838–1848. PubMed.
- AAA Foundation for Traffic Safety (2024). Drowsy Driving in Fatal Crashes, United States, 2017–2021.
- Hafner, M., Stepanek, M., Taylor, J., Troxel, W.M. & van Stolk, C. (2017). Why Sleep Matters — The Economic Costs of Insufficient Sleep: A Cross-Country Comparative Analysis. RAND Health Quarterly 6(4):11. Research brief.
- Watson, N.F., Badr, M.S., Belenky, G., et al. (2015). Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Journal of Clinical Sleep Medicine 11(6):591–592. PMC.
- Hirshkowitz, M., Whiton, K., Albert, S.M., et al. (2015). National Sleep Foundation's sleep time duration recommendations: methodology and results summary. Sleep Health 1(1):40–43. PubMed.
- Rosekind, M.R., Graeber, R.C., Dinges, D.F., et al. (1995). Crew Factors in Flight Operations IX: Effects of Planned Cockpit Rest on Crew Performance and Alertness in Long-Haul Operations. NASA Technical Memorandum 108839. NASA NTRS.
- CDC National Center for Health Statistics (2024). Short Sleep Duration and Sleep Difficulties Among Adults: United States, 2024. NCHS Data Brief No. 559. CDC.