Why Am I Tired After 8 Hours of Sleep? 11 Causes and a 4-Week Self-Check
Sleep inertia, late caffeine, OSA, social jet lag, and the other usual suspects — with a four-week self-screening plan and clear thresholds for seeing a doctor.
This is an informational summary of peer-reviewed sleep medicine research. It is not medical advice, diagnosis, or treatment recommendation. The lists of causes and markers below are intended to inform a conversation with a clinician — they are not diagnostic tools. If you have persistent fatigue or suspect a sleep disorder, please consult a licensed healthcare professional.
Eleven PM bedtime, 7 AM wake, eight solid hours by the tracker. So why does standing up feel like wading through wet cement, and why does it take two cups of coffee to feel human? If you're tired after 8 hours of sleep, the problem is almost never the eight hours itself. It's one of about eleven other things — most of them fixable, a few of them worth a doctor's attention.
This post starts with the most common reason (sleep inertia, the temporary morning fog), separates "tired" from two related-but-different states, walks through the eleven well-documented causes worth ruling out, and ends with a four-week self-check plan plus clear flags for when to escalate from self-help to medical evaluation.
The most common reason: sleep inertia
If "tired after 8 hours of sleep" mostly means the first 30–60 minutes after waking feel foggy and slow, the answer is probably sleep inertia. Sleep inertia is a defined clinical phenomenon — "the temporary time of sleepiness, disorientation, and impaired cognitive performance experienced upon awakening" (Hilditch & McHill 2019 review). It happens to nearly everyone every morning. The question is just how much of it you experience and how long it lasts.
The numbers worth knowing:
- Subjective duration: typically 15–30 minutes, with full recovery within an hour for most people. Under chronic sleep restriction, performance can fail to reach baseline at 70 minutes post-waking.
- Cognitive performance can take longer than it feels: reviews report measurable performance lag of up to 2 to 3.5 hours for complex tasks, even when subjective alertness is back to normal much sooner.
- The brain wakes up unevenly: brainstem and thalamus reactivate near-instantly, but anterior cortical regions — including the prefrontal cortex — take longer to return to baseline activation. Cerebral blood flow can stay below pre-sleep levels for around 30 minutes.
- What stage you wake from matters: waking from N3 (deep slow-wave sleep) produces a notable performance drop compared with waking from lighter stages — one cited lab study reported a 41% reduction after SWS waking versus near-zero after N2 waking.
So if you sleep 8 hours but the alarm catches you 30 minutes into a sixth cycle (deep in N3), the next 60–90 minutes feel rough — not because you didn't sleep enough, but because you woke from the wrong stage. Five clean cycles ending right at the alarm (7.5 hours) often feels better than 8 hours that ends mid-cycle. The mechanics of why are covered in How Sleep Cycles Work; the practical fix — backing into a cycle-aligned bedtime — is in What Time Should I Go to Bed if I Wake at 6 AM?
What actually helps with sleep inertia (per the evidence):
| Approach | Evidence | Notes |
|---|---|---|
| Cycle-aligned wake (avoid waking from N3) | Strong | The clearest fix. Use the Sleep Cycle Calculator to find a bedtime that lands the alarm in lighter sleep. |
| Pre-nap caffeine (~100–200 mg, 30 min before) | Good | Reduces post-nap inertia, though benefit is measurable about 15 minutes after waking, not immediately (PMC5136610). |
| Reactive caffeine (drinking coffee after the alarm) | Slow | Vigilance effects are detectable around 12–18 minutes after intake. The first 10 minutes will still feel foggy. |
| Bright light (e.g., 2,000 lux for 1 minute) | Subjective only | Improves how you feel, but controlled trials show no objective performance gain in the first 15 minutes. |
| Cold water on the face | Subjective only | Can produce a false sense of alertness without measurable performance recovery. |
| "Adrenaline kicks in" | No evidence | Repeated online; no controlled studies support this as an inertia countermeasure. |
The single highest-leverage move is changing what stage you wake from — and that's bedtime, not the morning routine.
"Tired" means three different things
Doctors usually start by asking which version of tired you mean, because each points to a different cause and a different fix.
- Sleepy: nodding off in conversations, fighting your eyes during meetings, falling asleep within seconds when you sit down. This is a strong signal of insufficient sleep, undiagnosed sleep apnea, or a circadian misalignment.
- Tired: low energy, low motivation, "could really use a coffee" but not actually falling asleep. Often a lifestyle pattern — caffeine timing, exercise, hydration, or schedule consistency.
- Fatigued: chronically depleted regardless of how much you sleep, with the feeling that even rest doesn't restore you. This usually points to a medical cause — thyroid, iron, B12, depression, or chronic disease — and warrants evaluation.
Clinical literature commonly associates the sleepy presentation with sleep inertia or undiagnosed apnea, the tired presentation with lifestyle factors discussed in the next section, and persistent fatigue over weeks with conditions warranting medical evaluation. The distinction is described in sleep medicine intake as a triage starting point — not a self-diagnostic conclusion.
Eleven common causes worth ruling out
The following list is broadly ordered by prevalence. Each row describes the cause, mechanism, and the markers clinical literature commonly associates with it — intended to inform a conversation with a clinician rather than as a self-diagnostic tool.
| # | Cause | Markers worth raising with a clinician |
|---|---|---|
| 1 | Undiagnosed obstructive sleep apnea (OSA) | Loud snoring + observed apneas + neck circumference >40 cm + BMI >30 + age >50 → take the STOP-BANG questionnaire. The original Wisconsin cohort (Young 1997) estimated that the majority of moderate-to-severe OSA in adults goes clinically undiagnosed. |
| 2 | Restless legs / periodic limb movement (PLMS) | Unpleasant leg sensations relieved by movement, evening worsening, partner reports kicking. Low ferritin (<75 ng/mL) raises risk. |
| 3 | Circadian misalignment / social jet lag | Weekday vs. weekend wake times differ by ≥2 hours; "Monday morning is the worst" is the lived experience. Evening chronotypes forced onto early schedules report fatigue even with adequate sleep opportunity (PMC8707256). |
| 4 | Late-day caffeine | Caffeine after early afternoon + still tired in the morning. Caffeine has a half-life of 5–6 hours on average (range 2–12). A controlled trial found that 400 mg of caffeine taken even 12 hours before bedtime measurably reduced N3 deep sleep (PMC11985402). The fatigue may itself be the caffeine. |
| 5 | Alcohol — even 1–2 drinks | Evening drinking + waking at 3–5 AM. Alcohol delays REM onset and fragments second-half sleep; clearer first-half REM suppression appears mainly at higher doses (Ebrahim 2013). |
| 6 | Mild dehydration | Concentrated morning urine + dry mouth + low-grade headache. A 1–2% body-weight fluid loss measurably reduces alertness and increases reaction time (PMC4207053). |
| 7 | Low ferritin / B12 / iron | Cold extremities + restless legs at night + fatigue despite adequate sleep. Ferritin below 75 ng/mL is the consensus threshold flagged by the RLS Foundation Medical Advisory Board for restless-legs symptoms; check ferritin, full CBC, and B12 if symptomatic. |
| 8 | Subclinical hypothyroidism | Cold intolerance + weight gain + fatigue + dry skin. Affects roughly 3–15% of adults overall, rising to 18–20% in older adults (StatPearls). A simple TSH blood test screens for it. |
| 9 | Depression or anxiety | Waking 2–3 hours before the alarm + low mood for two weeks or longer. Depression alters sleep architecture: shortened REM latency, increased REM density, reduced slow-wave sleep, early-morning awakening (PMC6386825). |
| 10 | Sleep environment | Bedroom warmer than around 22 °C / 72 °F, ambient light leaking in, partner snoring. Studies in older adults show a 5–10% drop in sleep efficiency as bedroom temperature rises from 25 °C to 30 °C (effect size in younger adults is likely smaller but in the same direction). |
| 11 | Medications | Started a new prescription in the last 6–12 weeks coinciding with new fatigue. Common offenders: SSRIs (REM suppression and increased REM latency, well-documented in reviews of antidepressant effects on sleep), beta-blockers like propranolol (Stoschitzky 1999 documented up to 80% reduction in nighttime melatonin), and first-generation antihistamines (next-day grogginess from H1-receptor occupancy persisting into the morning, e.g. Zhang 2010). Talk to the prescriber about timing and alternatives — don't stop on your own. |
Common factors a clinical workup explores first
Sleep medicine intake commonly works through the following factors in approximately this order — beginning with caffeine, alcohol, and bedroom environment because these are the highest-yield modifiable variables in the literature, then cycle alignment, then more specialized investigation. The sequence below describes that workflow as informational reference, not as a self-administered protocol; whether and how it applies to a specific person is a clinical decision.
Week 1 — environment and stimulants. Cut caffeine by noon. No alcohol for the full week. Bedroom temperature 18–20 °C. Blackout curtains or a sleep mask. White noise or earplugs if there's any ambient noise. This handles four of the eleven causes simultaneously and is the highest-yield first move.
Week 2 — cycle alignment and consistent schedule. Use the Sleep Cycle Calculator to back into a bedtime that aligns the alarm with the end of a cycle. Hold weekday and weekend wake times within 30 minutes of each other to neutralize social jet lag. Most readers see noticeable improvement just from these two changes:
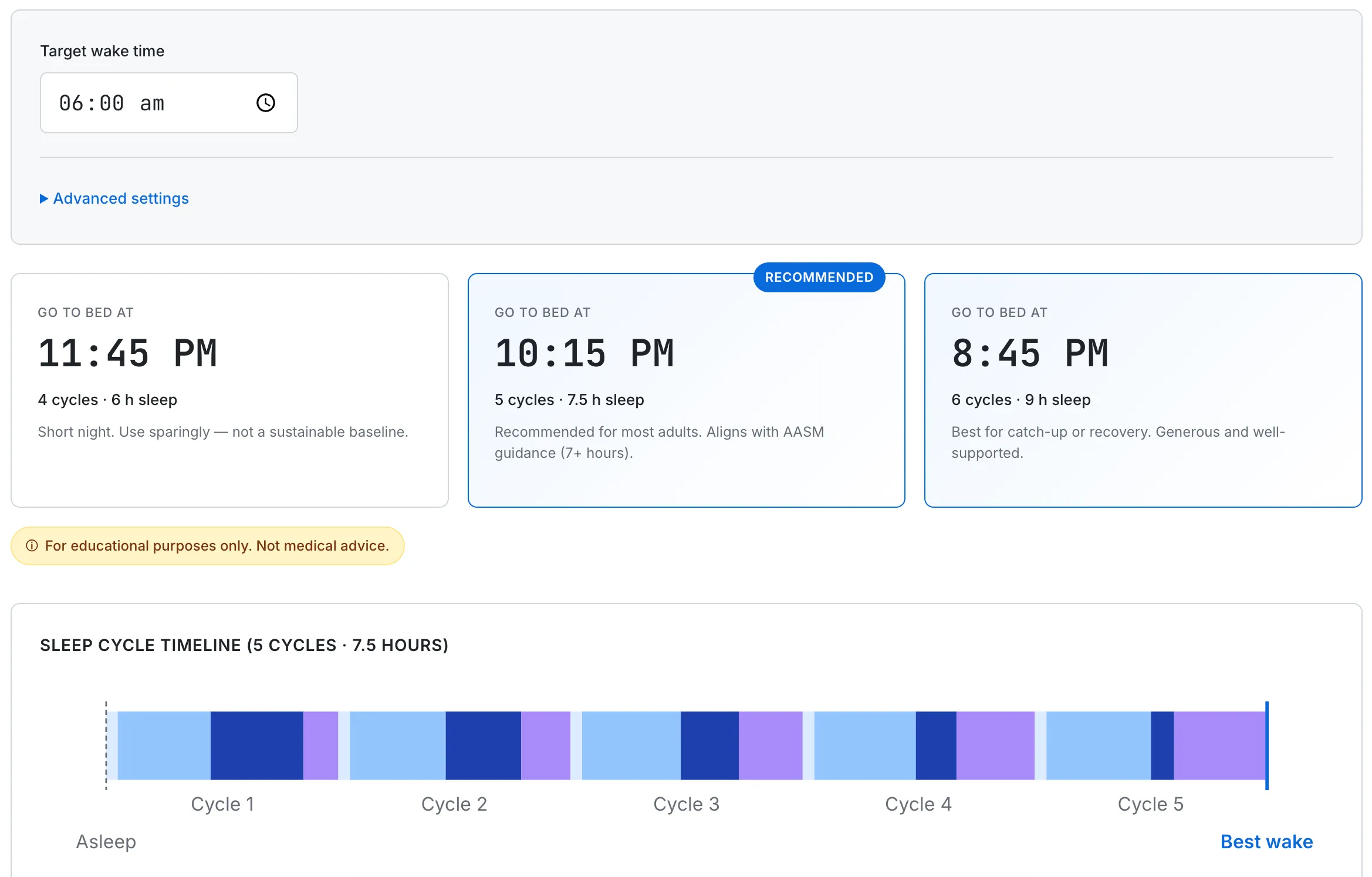
Working back from a 6 AM wake target, the calculator shows three cycle-aligned bedtimes: 11:45 PM (4 cycles), 10:15 PM (5 cycles, recommended), and 8:45 PM (6 cycles). Cycle length and onset time are adjustable for personal calibration.
Week 3 — self-screening if Week 1 and 2 didn't fix it. Take the STOP-BANG questionnaire. If you score 3 or higher, ask a primary-care doctor about a sleep study. Get a basic blood panel: TSH, ferritin, vitamin B12, vitamin D. If you started any new medication in the last six weeks, check the side-effect profile for sleep disruption.
Week 4 — clinical follow-up if needed. Take the lab results and STOP-BANG score to a primary-care provider or sleep specialist. Persistent fatigue after addressing Weeks 1–3 is a real signal, not laziness or "just being tired." A sleep study is the gold standard for ruling in or out OSA, RLS, and several other sleep disorders.
When to skip the four weeks and see a doctor now
Some symptom combinations don't deserve four weeks of self-experimentation. Escalate to medical evaluation immediately if any of the following apply:
- Loud snoring + witnessed pauses in breathing + daytime sleepiness. Strong indicator of OSA; warrants a sleep study.
- Falling asleep involuntarily during conversations, meetings, or — most importantly — driving. An Epworth Sleepiness Scale score of 10 or higher is the standard cutoff.
- Persistent unrefreshing sleep for more than three weeks despite addressing caffeine, alcohol, schedule, and bedroom environment.
- Fatigue with cold intolerance, weight change, or hair thinning. Order TSH, ferritin, B12, and vitamin D.
- Early-morning awakening + low mood or anhedonia for two weeks or more. Screen for depression with PHQ-9.
- New medication started in the last 6–12 weeks coinciding with new fatigue. Review with the prescriber — don't stop on your own.
The eleven causes above cover the great majority of "tired after 8 hours" complaints. Most are solvable with lifestyle changes; a few need a doctor; a small fraction need a sleep specialist. The goal of the four-week plan is to figure out which bucket you're in without spinning your wheels.
This guide describes general adult sleep medicine drawn from peer-reviewed sources and is for educational use only. Individual sleep needs, cycle lengths, and medical conditions vary. None of this is medical advice or a substitute for a clinical evaluation. If you have ongoing trouble sleeping, suspect a sleep disorder, or experience persistent fatigue despite addressing the common causes above, please consult a licensed healthcare professional.