Is 6 Hours of Sleep Enough? What the Research Actually Shows
Most adults who feel fine on six hours don't notice the cognitive cost. The honest read on what published sleep research says, and the narrow categories where six hours might genuinely be enough.
This is an informational summary of peer-reviewed sleep research and major guideline statements on adult sleep duration. It is not medical advice, diagnosis, or treatment guidance. The studies cited describe controlled lab conditions or population cohorts — not personal predictions, and individual sleep need varies with age, health, medications, and underlying conditions. If persistent insomnia, daytime sleepiness, or unrefreshing sleep is affecting your day, please consult a licensed healthcare professional.
In 2003, a Penn State team led by Hans Van Dongen restricted healthy young adults to 6 hours of sleep per night for 14 consecutive nights and tracked their cognitive performance. By the end of the two weeks, the 6-hour group performed about as poorly on attention and working-memory tests as people who had stayed awake for two straight nights — and the participants in the 6-hour group did not notice. Their subjective sleepiness ratings plateaued after a few days. They felt adapted. Their brains had not adapted. They had simply stopped registering the deficit.
This post walks through five things — (1) what the major sleep guidelines actually classify at six hours, (2) what cohort and randomized data show in chronic 6-hour sleepers, (3) why "I feel fine on six" is a self-report you can't fully trust, (4) the narrow categories where 6 hours might genuinely be enough, and (5) practical signals you can use to estimate where you sit, without a sleep lab.
Is 6 hours of sleep enough? What the major guidelines classify
The American Academy of Sleep Medicine (AASM) and the Sleep Research Society released a joint consensus statement in 2015 covering the recommended sleep duration for adults aged 18 to 60. The panel reviewed evidence across nine health domains — general health, cardiovascular, metabolic, mental health, immune, performance, cancer, pain, and mortality — and concluded that adults should sleep at least 7 hours per night on a regular basis. The exact wording on the lower end was specific — "There was consensus that 6 hours of sleep or less was inappropriate to support optimal health." Consensus could not be reached on the 6-to-7-hour band itself, but the median panel vote placed it in the inappropriate category as well (Watson et al. 2015).
The National Sleep Foundation (NSF) reached similar conclusions in 2015, with slightly softer category labels. For adults aged 18 to 64, the NSF recommends 7 to 9 hours, lists 6 hours as "may be appropriate" — a deliberately uncertain middle category — and lists less than 6 hours as "not recommended." For adults 65 and older, the recommended range drops to 7 to 8 hours, with 5 to 6 hours treated as "may be appropriate" (Hirshkowitz et al. 2015).
The CDC aligns with the AASM at 7 or more hours per 24 hours. The CDC's most recent National Health Interview Survey data put 30.5% of US adults under that 7-hour threshold (NCHS Data Brief 559, 2024) — meaning about one in three adults is below the level the major bodies of sleep medicine treat as the floor for healthy adult sleep.
The point worth carrying through the rest of this article — for most adults under 65, the major bodies of sleep medicine describe 6 hours as either inappropriate or in a hedged middle zone. The recommended zone starts at 7 hours, not 6.
What 6-hour nights look like in the data — Cappuccio, Van Dongen, Whitehall II
Three lines of evidence repeatedly show up when researchers describe what 6-hour nights actually do over time — population mortality cohorts, randomized lab restriction, and longitudinal cognitive cohorts. Each measures something different.
Cappuccio 2010 — population mortality. The 2010 meta-analysis by Francesco Cappuccio and colleagues pooled 27 prospective cohort studies with 1,382,999 participants. Short sleepers (typically defined as under 7 hours per night) showed an all-cause mortality relative risk of 1.12 (95% CI 1.06–1.18) versus the reference range. Long sleepers (over 9 hours) showed a stronger association, RR 1.30 (1.22–1.38), but the long-sleep signal in cohort data is heavily confounded by underlying illness driving long sleep, rather than the reverse. The honest read on Cappuccio is that 6 hours is not a fatal number — the effect size sits below smoking and obesity in magnitude — but the curve is real, monotonic, and replicated across cohorts, and the dose-response steepens below 5 hours per night.
Van Dongen 2003 — randomized cognitive restriction. The clearest experimental data on chronic 6-hour nights come from the Van Dongen 2003 Penn State trial. Healthy adults were randomized into 4-, 6-, or 8-hour sleep groups for 14 consecutive nights, with daily psychomotor vigilance, working memory, and addition tasks. By day 14, participants in the 6-hour group showed cumulative deficits — in the authors' published phrasing — "equivalent to up to 2 nights of total sleep deprivation." The deficit was dose-dependent and showed no asymptote across the two weeks. The 4-hour group reached the same deficit faster.
Belenky 2003 — sleep restriction stabilization. Belenky and colleagues ran a similar protocol with 3-, 5-, 7-, and 9-hour sleep groups across 7 nights. Performance in the 5-hour group declined initially and then "stabilized at a reduced level" — not at baseline. The literature describes this stabilization as the brain accommodating reduced function rather than recovering it, and a person living through the pattern would experience the lower steady state as their new normal.
Whitehall II — long-term cardiovascular and cognitive cohorts. The British civil-servant Whitehall II cohort followed thousands of adults over years. Among those sleeping 6, 7, or 8 hours at baseline whose sleep duration decreased over the next several years, the cardiovascular mortality hazard ratio reached 2.4 (95% CI 1.4–4.1; Ferrie 2007). The companion cognitive analysis reported that adverse changes in sleep duration were associated with declines in reasoning, vocabulary, and the MMSE — with the magnitude of those effects on the order of 4 to 7 years of additional cognitive aging (Ferrie 2011). Mechanisms behind why people often feel tired even after a full night of sleep are covered in Why Am I Tired After 8 Hours of Sleep?
Why "I feel fine on six hours" is a self-report you can't fully trust
The Van Dongen 2003 result has a second layer that often goes unmentioned. While objective cognitive performance kept degrading day after day in the 6-hour group, subjective sleepiness ratings plateaued after a few days. Participants felt that they had adapted. They had not — they had simply stopped noticing the deficit. Van Dongen wrote it directly in the paper — "Sleepiness ratings suggest that subjects were largely unaware of these increasing cognitive deficits, which may explain why the impact of chronic sleep restriction on waking cognitive functions is often assumed to be benign."
The CARDIA Sleep Study (Lauderdale et al. 2008) corroborated the gap from a different angle. Comparing self-reported sleep duration with actigraphy in 669 participants, the correlation was r = 0.45. People over-reported their sleep by an average of about 0.80 hours — meaning a person who reports sleeping 7 hours often slept closer to 6.2 hours measured.
Belenky 2003 added the stabilization finding — performance stabilized at a reduced level, not at baseline. A person living through that pattern would experience the lower steady state as their new normal, indistinguishable from feeling fine at full function.
Taken together — if you sleep 6 hours and feel fine, that subjective state is not strong evidence that 6 hours is enough for you. It may simply be evidence that your brain has stopped registering the deficit it's carrying.
Where 6 hours might genuinely be enough — narrow categories with sources
Three small sub-populations are worth being honest about — the conditions under which 6 hours could genuinely be sufficient.
Adults 65 and older. The NSF 2015 categorized 5 to 6 hours as "may be appropriate" for adults 65+, with 7 to 8 hours as the recommended range. The National Institute on Aging makes a key distinction in its publicly facing materials — older adults' sleep need does not drop with age, but their ability to maintain consolidated nighttime sleep often declines, often through sleep architecture fragmentation and concurrent conditions like sleep apnea or restless legs. Practical implication — a 70-year-old reporting 6 hours of nighttime sleep is not necessarily a healthy baseline, and the literature describes that scenario as worth investigating the night, rather than accepting the number as a healthy adaptation.
Familial natural short sleep (FNSS). A small set of families have been documented carrying mutations in genes that produce a shortened sleep need without measurable cognitive cost. Mutations identified to date span four genes — DEC2/BHLHE41 (He et al. 2009, Science), ADRB1 (Shi et al. 2019, Neuron), NPSR1 (Xing et al. 2019), and GRM1 (Shi et al. 2021). DEC2 carriers in the original He et al. report slept around 6.25 hours on average versus 8.06 hours in non-carriers. ADRB1 carriers were described as sleeping roughly two hours less per night than non-carriers within their families.
The honest read on prevalence — more than 50 FNSS families have been identified worldwide as of recent reviews, but biobank follow-up studies have generally not replicated the short-sleep phenotype in unrelated carriers of the same mutations (FNSS gene review, PMC8547374). That non-replication suggests the true population prevalence of the genuinely-fine-on-6h phenotype is likely lower than the 1–3% some popular secondary sources cite — it remains uncertain, but more conservative readings of the data place it well under 1%.
The phenotype itself is specific. People with FNSS typically report lifelong short sleep — not a recent pattern — voluntary, with a clear family history. They wake without alarms at around 6 hours, do not catch up on weekends, sustain alertness through the day without caffeine, and have normal BMI and mood profiles. Feeling adapted to 6 hours over the past year of working hard is not the same signal.
Exceptionally consolidated, high-efficiency sleep. A small literature on sleep quality versus quantity describes consolidated, high-efficiency, fragmentation-free 6 hours as potentially more restorative than fragmented 8 hours. The compensation is real but narrow — the same comparisons in the literature still describe 7 to 8 hours of comparable quality as superior to 6 hours of comparable quality (slow wave sleep review, PMC8304732).
Practical signals — how to estimate where you sit, without a sleep lab
This section is informational, not diagnostic. The signals below are described in the published literature as commonly suggestive of insufficient sleep — none of them, alone or together, replace a clinical evaluation.
Patterns commonly described as suggesting chronic insufficient sleep:
- You wake to 7 to 8 hours when no alarm is set. Vacation mornings or weekend mornings after no late commitments give a closer estimate of biological sleep need than weekday duration.
- Weekend sleep exceeds weeknight sleep by 2 hours or more. Persistent catch-up reflects accumulating sleep debt during the week. The weekend recovery question is covered in Can You Catch Up on Sleep on Weekends?
- You can fall asleep within 5 minutes of trying during the day. In clinical settings, the Multiple Sleep Latency Test classifies sleep latency under 8 minutes as objective excessive sleepiness; falling asleep on the sofa within 5 minutes of starting to read is an informal proxy.
- Morning fog and irritability without caffeine. Caffeine masking suggests dependence on a stimulant to reach baseline alertness — a pattern the literature describes as worth noticing.
- Increased craving for sweet or calorie-dense food and amplified emotional reactivity. Sleep restriction has been associated with elevated ghrelin, decreased leptin, and increased amygdala reactivity to negative stimuli.
- Difficulty with word retrieval, decision-making under load, and route-finding in unfamiliar areas. Prefrontal-cortex-dependent tasks tend to degrade earlier than motor tasks under chronic sleep restriction.
Signals that 6 hours could genuinely be enough — they need to all be present, not just one:
- Lifelong pattern of 5.5 to 6 hours of voluntary sleep, not a recent change.
- Clear family history of similar pattern.
- Wake without an alarm at around 6 hours.
- No tendency to catch up on weekends.
- Sustained daytime alertness without caffeine reliance.
- Normal BMI and mood baseline.
Patterns the clinical literature describes as worth a professional evaluation rather than self-management include unrefreshing sleep with loud snoring, persistent insomnia of 6+ months, persistent daytime sleepiness while driving, and depression with concurrent sleep changes. These framings are descriptive of how sleep medicine handles those scenarios — they are not directive about what any individual should do.
If you'd like to translate a target sleep duration into specific cycle-aligned bedtimes, the Sleep Cycle Calculator tool runs the math for any wake time, with adjustable cycle length and sleep onset latency.
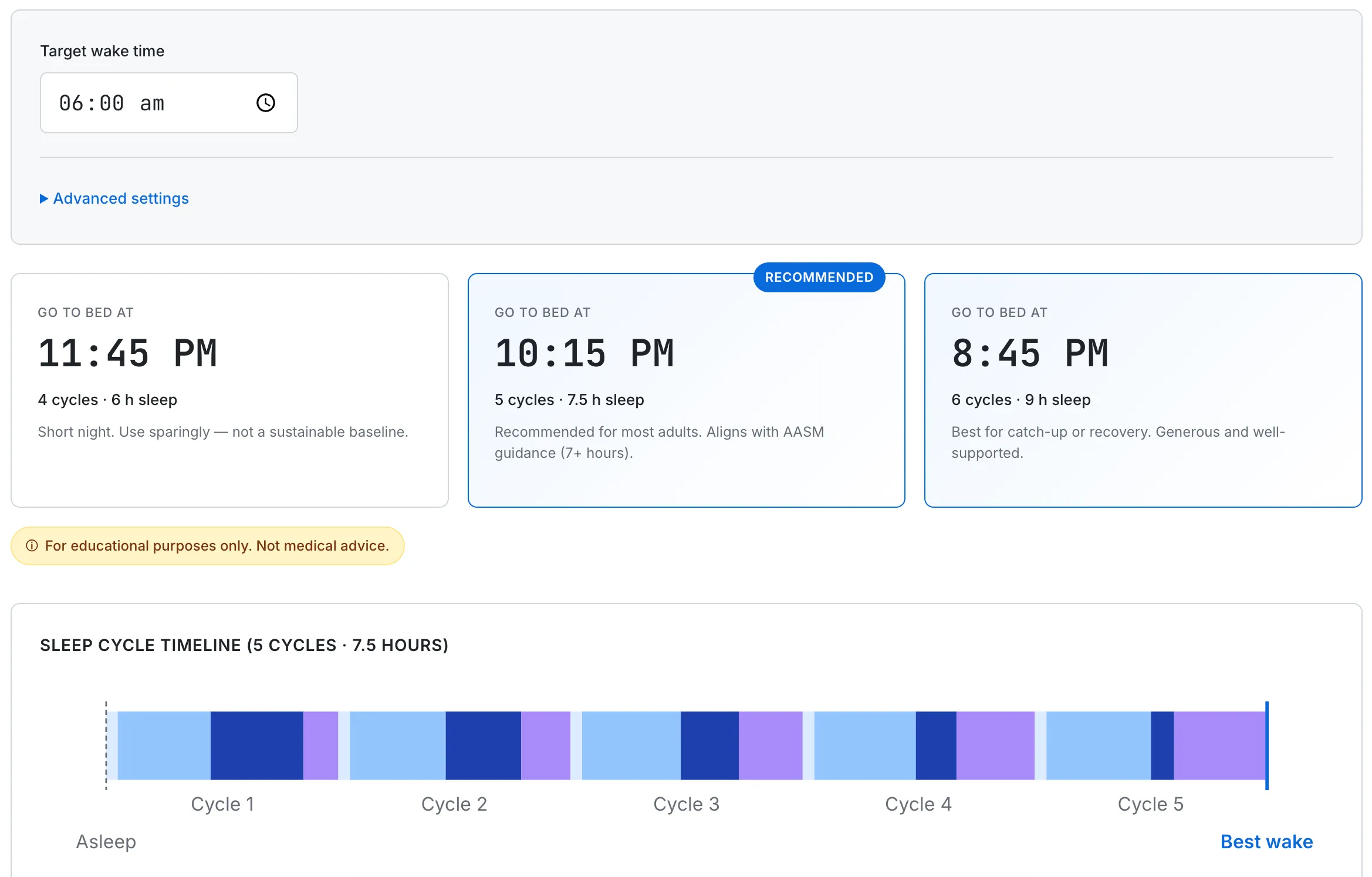
Mapping wake time onto cycle-aligned bedtimes inside the 7-to-9-hour recommended range. Cycle length and sleep onset latency are tunable for individual variation.
Frequently Asked Questions
Is 6 hours of sleep enough for an adult?
For most adults under 65, the major bodies of sleep medicine — AASM, NSF, CDC — describe 6 hours as inadequate or in a hedged "may be appropriate" middle zone, with the recommended range starting at 7 hours. The Watson et al. 2015 AASM/SRS consensus statement specifically used the wording "6 hours of sleep or less was inappropriate to support optimal health." Cohort and randomized data converge on the same picture for chronic adult use.
Why do I feel fine on 6 hours of sleep?
Subjective adaptation is real — and it is largely an illusion. Van Dongen 2003 showed that participants restricted to 6 hours per night plateaued in their subjective sleepiness ratings after a few days while their objective cognitive performance kept declining for two weeks. Belenky 2003 described the same pattern as performance "stabilizing at a reduced level" rather than recovering. Lauderdale 2008 separately found that people over-report their sleep by about 0.80 hours on average compared with actigraphy. "Feeling fine on six" is more often a perception failure than a biological adaptation.
Are short sleepers real?
Yes, but the genuine phenotype — familial natural short sleep (FNSS) — is rare. More than 50 FNSS families have been identified across four characterized gene mutations (DEC2/BHLHE41, ADRB1, NPSR1, GRM1), but biobank follow-ups have not consistently replicated the short-sleep phenotype in unrelated carriers of the same variants. True population prevalence is uncertain, and conservative readings of the data place it well under the 1–3% some popular secondary sources cite. The phenotype is specific — lifelong, voluntary, family history, no weekend catch-up, no caffeine reliance, normal BMI.
Can you train yourself to need less sleep?
The published literature does not describe this as a real phenomenon. Belenky 2003 showed that the brain stabilizes at a reduced level under chronic restriction — not that it recovers full function. Van Dongen 2003 showed that participants stop noticing their own deficit, not that the deficit disappears. The closest thing to "training" in the data is the perception of having adapted, which the same studies describe as the deficit going under the radar of self-awareness.
Is sleep regularity more important than sleep duration?
Recent work (Windred 2024, SLEEP, n=88,975 from the UK Biobank) suggests sleep regularity is at least as strong a mortality predictor as duration, with the top regularity quintile showing 20–48% lower all-cause mortality. The honest read is not that duration stops mattering — both matter — but that going to bed and waking at consistent times appears comparable in importance to hitting the recommended duration.
Is 5 hours of sleep enough?
The literature is more uniform here. Watson 2015 explicitly classified less than 6 hours as inappropriate; NSF classified less than 6 hours as "not recommended" (with the small adjustment of "5 to 6 hours may be appropriate" for 65+ adults). Cappuccio 2010's mortality dose-response steepens below 5 hours, and randomized restriction studies (Van Dongen 2003, Belenky 2003) showed faster cognitive decline at 4-hour and 5-hour conditions versus 6 hours. Five hours of sleep is described in published evidence as more clearly inadequate than six.
This guide summarizes general adult sleep medicine drawn from peer-reviewed sources and major guideline documents. The associations described above (mortality, cardiovascular risk, cognitive decline) come from observational and short-term experimental studies — they describe statistical patterns at the population level, not personal predictions. None of this is medical advice or a substitute for clinical evaluation. If you have ongoing sleep difficulty, suspect a sleep disorder, or are concerned about sleep-related symptoms, please consult a licensed healthcare professional.