How Many Hours of Sleep Do You Need by Age? A 2026 Guide Backed by CDC, AASM, and the National Sleep Foundation
The chart is everywhere. Here's the part the chart doesn't show — what changes with pregnancy, shift work, and aging, and why "I'm fine on six" usually isn't.
This is an informational summary of clinical guidelines (CDC, AASM, NSF, NIA) and peer-reviewed sleep research. It is not medical advice. Recommended hours describe population-level guidance; individual needs vary with age, pregnancy, illness, shift work, and other factors. If you have concerns about your own or a family member's sleep, please consult a licensed healthcare professional.
Recommended-sleep charts by age are everywhere online. The trouble is what they leave out. One common belief — especially among older adults — is that you need less sleep as you age. But on the National Institute on Aging's own website, that idea is explicitly listed as a myth: someone at seventy isn't supposed to sleep less, and sleep that shrinks with age is itself often a warning sign, not a milestone. The chart also can't see the rest of your life — the same person at thirty needs roughly 30 to 60 minutes more sleep in the first trimester of pregnancy.
This post walks through (1) the per-age recommendations from newborns to 65+, (2) why the CDC, AASM, and NSF subtly differ, (3) the variables the standard chart leaves out — pregnancy, illness, shift work, jet lag — and (4) the self-check for whether you're actually getting enough, which matters more than the number.
Sleep needs by age — the full chart
The recommendations come from expert panels at the AASM (American Academy of Sleep Medicine) and the NSF (National Sleep Foundation), each having reviewed thousands of papers. The CDC publishes a simplified version for the general public.
| Age group | Recommended hours | Source |
|---|---|---|
| Newborn 0–3 months | 14–17 hours (incl. naps) | NSF; aligned with AAP |
| Infant 4–12 months | 12–16 hours (incl. naps) | AASM / CDC |
| Toddler 1–2 years | 11–14 hours (incl. naps) | AASM / CDC |
| Preschooler 3–5 years | 10–13 hours (incl. naps) | AASM / CDC |
| School-age 6–12 years | 9–12 hours | AASM / CDC |
| Teen 13–17 (CDC) / 13–18 (AASM) | 8–10 hours | AASM / CDC |
| Adult 18–60 | At least 7 hours (recommended 7–9) | CDC; AASM/SRS 2015 |
| Adult 61–64 | 7–9 hours | CDC |
| 65+ | 7–8 hours | CDC (NIA: 7–9 hours) |
Three things to know about the chart:
- The AASM and the CDC use the same pediatric numbers — both adopt the Paruthi 2016 consensus.
- The NSF's adult range (7–9 hours) is narrower than the CDC's "at least seven."
- For ages 5 and under, those hours include daytime naps. Getting all 14 hours from one overnight stretch isn't realistic.
Why the three major bodies don't always agree
The CDC, AASM, and NSF look at the same underlying evidence and produce slightly different recommendations. The reason is methodology.
- AASM/SRS consensus (Watson 2015): A 15-member expert panel reviewed 5,314 papers across nine health domains — cardiovascular, metabolic, mental health, immune, cognitive performance, cancer, pain, and mortality among them — and reached a consensus by structured vote. For adults 18–60, the conclusion was "at least seven hours" for health, with nine or more potentially appropriate during recovery or developmental periods.
- NSF recommendation (Hirshkowitz 2015): An 18-scientist panel using a similar process. The NSF adds an explicit recommended range (7–9 hours) and, separately, a per-age-band may-be-appropriate range that extends as low as six hours and as high as ten or eleven — listed as discrete cells, not as a single continuous range.
- CDC: A simplified summary of those two consensus efforts for the general public. The CDC table ends at "at least seven hours" for adults; the original AASM and NSF documents include more graded categories.
The bottom line — every major body agrees that seven hours is the adult floor. Where they diverge is on how high the upper end goes, and how much variation to call normal.
Adults 18–64: why "7 hours" is the floor, not the goal
The phrase "seven hours is enough" is often misread. Seven hours isn't the goal — it's the minimum.
A 2025 meta-analysis in GeroScience pooled large adult cohorts and looked at all-cause mortality relative to people sleeping 7–8 hours per night:
- Less than 7 hours: 14% higher mortality (HR 1.14)
- 9 or more hours: 34% higher mortality (HR 1.34)
A U-shaped curve. Short sleep is risky, and so is long sleep — though the elevated risk on the long end is at least partly driven by underlying illness rather than caused by long sleep itself, since chronic disease tends to lengthen sleep.
The "I'm fine on six" claim is rarely true. People with the DEC2 (BHLHE41) gene variant can sleep around six hours with no measurable cognitive or metabolic deficit, and this trait is estimated at roughly 1–3% of the population. Before assuming you're in that 1–3%, it's worth knowing that most "I do fine on six" self-assessments are something else — adapted desensitization to sleep debt.
A 2003 SLEEP study by Van Dongen et al. nailed this directly. After 14 nights of six hours per night, participants' cognitive performance had dropped to the level of two consecutive nights without sleep — but the participants themselves didn't notice. The most dangerous kind of sleep deprivation is the kind that feels normal because you've stopped registering it. (More on the felt experience side of this in Why Am I Tired After 8 Hours of Sleep?)
Adults 65+: the "less sleep with age" myth
The National Institute on Aging is explicit — adults 65 and older still need about seven to nine hours per night. Sleep getting shorter with age is not a healthy adaptation.
So why does sleep often look shorter in older adults? Three things happen at once:
- Sleep fragmentation. More mid-night awakenings, which lowers the recorded total even when the time in bed hasn't changed.
- Phase advance. A shift toward earlier bedtimes (8–9 PM) and earlier wake times (4–5 AM). The clock moves; the duration may not.
- Less N3 (deep sleep). Even at the same total, recovery quality drops, so seven hours can feel less restorative.
These three are signals to focus on sleep quality, not to lower the target hours. If a parent in their seventies says "I'm fine on five hours" but is also showing reduced daytime energy, mood changes, or rising blood pressure, those changes warrant a real evaluation rather than being chalked up to age.
Children and teens: why developing brains are different
The recommendations for children and teens are listed in the chart above. The reality is well below them.
- According to CDC data, about 77% of US high schoolers don't get the recommended eight hours on a school night.
- Teen drivers sleeping less than eight hours are about 33% more likely to crash than peers getting eight or more (CHOP analysis).
- One school district in Wyoming (Jackson Hole High School) shifted its start time to 8:55 AM — and teen crashes dropped by up to 70% (Wahlstrom et al., CAREI multi-site study).
The American Academy of Pediatrics recommends middle and high schools start no earlier than 8:30 AM (2014 policy statement). Adoption is uneven, but parents control a few important variables anyway: a stable weekday bedtime, no screens in the bedroom, and — most underrated — keeping the gap between weekday and weekend wake times within two hours. That last one is the teen-specific defense against social jet lag, which compounds quickly.
When sleep needs change: pregnancy, illness, shift work, travel
The chart assumes a healthy average. Several common situations push the real need higher.
- First-trimester pregnancy. Average nightly sleep tends to rise by roughly 30 minutes to an hour relative to pre-pregnancy (NSF). Hormonal shifts (a sharp rise in progesterone) and metabolic load are the main drivers; someone who slept six hours pre-pregnancy may now need closer to eight to feel functional.
- Illness and recovery. While the immune system is active, total sleep need can rise by 1–2 hours. Nine hours during a cold isn't oversleeping — it's the body doing its job.
- Shift work. A daytime sleep after a night shift averages 1–2 hours shorter than a regular night sleep. Hitting the recommended total over a 24-hour cycle usually means primary sleep + nap, not one consolidated stretch.
- Jet lag. After a 6-hour eastward shift, even seven hours of sleep is lower-quality for the first few days because REM is poorly distributed. Padding by 30 minutes for several nights helps. (If meetings cross time zones regularly, the World Clock can show overlapping work-hour windows.)
If any of these describes your situation, the chart is a baseline — your actual need is the chart plus a margin.
Quantity vs quality: how to tell if you're actually getting enough
Eric Zhou at Harvard Medical School puts it well — "if you awaken refreshed and feel like you have the energy to get through your day, then I would worry less about the exact number of hours you're sleeping" (Harvard Health). What the clock says matters less than whether you can wake naturally and stay alert through the morning without caffeine props.
Markers commonly described in sleep medicine as worth raising with a clinician (intended to inform a conversation, not as a self-administered diagnostic tool):
- Without an alarm, do you sleep an extra hour or more than usual? → Possible chronic deficit.
- Do you sleep two or more hours longer on weekends than weekdays? → Building social jet lag.
- Do you have heavy 2–4 PM drowsiness every day? → Could be afternoon dip, but it's also a common signal of nighttime under-sleeping.
- Have you experienced microsleep while driving or in meetings? → Not optional. Check your sleep total now.
- Can you focus through morning work without coffee? → If not, you may be coffee-dependent because of sleep, not the other way around.
Multiple positive markers in the list above are commonly described as a signal worth a clinical sleep evaluation, with attention to both quality (waking, environment, alcohol, caffeine timing) and quantity (the total hours). The chart is a population-level starting point — actual energy on a given day is the more accurate individual signal, and persistent issues warrant a clinician's review.
Once you know your target hours, the next question is what time should you actually be in bed. That depends on your wake time and the 90-minute sleep cycle. For a 7 AM alarm, 10:15 PM (5 cycles, 7.5 hours) or 8:45 PM (6 cycles, 9 hours) lands the alarm at the end of a cycle rather than mid-cycle — which is why people sleeping the same number of hours can feel very different. Cycle-aligned bedtimes for other wake times are worked out in What Time Should I Go to Bed if I Wake Up at 6 AM?. You don't have to do the math by hand.
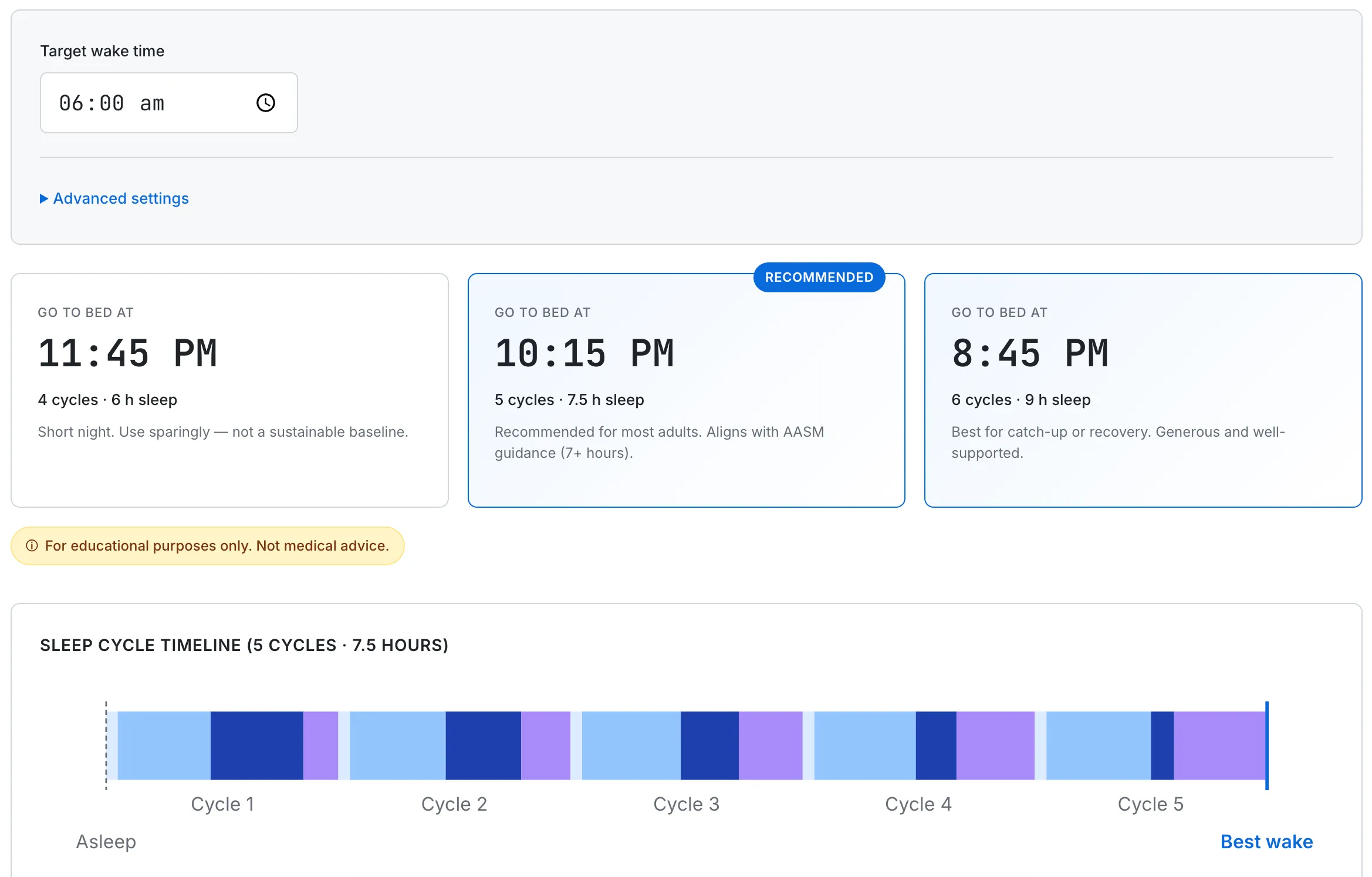
From a 7 AM wake target, the calculator shows two cycle-aligned bedtimes: 10:15 PM (5 cycles, 7.5 hours) and 8:45 PM (6 cycles, 9 hours). Cycle length and onset time can be tuned for individual variation.
Frequently Asked Questions
How many hours of sleep do adults need?
Adults 18 and over need at least 7 hours of sleep per night, with 7–9 hours the range most commonly recommended (CDC, the 2015 AASM/SRS consensus, and the National Sleep Foundation). The same applies to adults 65 and older.
Do adults over 65 need less sleep?
No. Adults 65 and older still need around 7–8 hours per night (the National Institute on Aging cites 7–9). The belief that you need less sleep as you age is explicitly listed as a myth by the National Institute on Aging — sleep that shrinks with age is often a warning sign, not a normal milestone.
How many hours of sleep do teenagers need?
Teenagers aged 13 to 18 need 8–10 hours of sleep per night, according to the AASM and the CDC, which both adopt the Paruthi 2016 pediatric consensus.
How much sleep do school-age children need?
School-age children aged 6 to 12 need 9–12 hours per night. Preschoolers (3–5) need 10–13 hours and toddlers (1–2) need 11–14 hours, including daytime naps.
Is 6 hours of sleep enough for an adult?
For most adults, no. Six hours falls below the recommended minimum of at least 7 hours per night (CDC; AASM/SRS 2015), with 7–9 hours the range most often advised.
This guide summarizes general adult and pediatric sleep medicine drawn from peer-reviewed sources and consensus statements, and is for educational use only. Individual sleep needs vary. None of this is medical advice or a substitute for a clinical evaluation. If you have ongoing trouble sleeping, suspect a sleep disorder, or have concerns about your child's or an older relative's sleep, please consult a licensed healthcare professional.