How to Fall Asleep Faster: What Research and Clinical Guidelines Describe
The AASM's 2021 guideline gives only one Strong recommendation for chronic insomnia. Here's what the research describes — clearly distinguishing clinical evidence from popular techniques.
This is an informational summary of peer-reviewed sleep research and clinical guidelines. It is not medical advice, diagnosis, or treatment recommendation. Some clinical protocols described below (such as sleep restriction therapy) carry safety considerations and are typically implemented under clinician supervision. If sleep difficulties affect your daily life, please consult a licensed healthcare professional.
It's 1 a.m. The alarm is set for 6:30. You convince yourself five and a half hours is enough — and thirty minutes later you check the clock again. 1:30. Tomorrow's meeting starts looping. You try 4-7-8 breathing — nothing. You think of the military sleep method, the one with the 96%-in-2-minutes claim. Still awake at 4.
Most "10 ways to fall asleep faster" articles list the military method, 4-7-8 breathing, and cognitive shuffle right next to clinically validated CBT techniques as if they were equivalent. They aren't.
This article walks through (1) what normal sleep onset looks like, (2) why trying harder tends to backfire — the sleep effort paradox, (3) the multicomponent CBT-i package as described by the 2021 guideline, (4) the Conditional-grade tools, (5) an honest read on popular techniques, (6) environment and timing — what research describes as the strongest single variable, and (7) when research describes escalation to a clinician.
This article is an informational summary of clinical sleep medicine literature, not individual medical advice. Please consult a clinician before applying any of this to your own situation.
How long should it take to fall asleep?
It helps to recalibrate expectations first. Normal sleep onset latency is generally described as 10–20 minutes. Falling asleep within five minutes is more often a sign of sleep deprivation than of being well-rested — the body is craving sleep that aggressively. Routinely needing more than 30 minutes is a different conversation, covered in the escalation section below.
The "fall asleep in 10 seconds" framing popular online conflicts with the underlying biology. Melatonin release → core body temperature drop → progression through REM and NREM stages plays out on a minutes-long cascade. The goal isn't artificially compressing this — it's removing the things that delay it.
Reference benchmarks:
- 5–10 minutes — fast (often interpreted as high sleep pressure)
- 10–20 minutes — typical
- 20–30 minutes — slower end of normal
- More than 30 minutes, often — worth checking against the DSM-5 chronic insomnia criteria below
Why trying harder makes it worse — the sleep effort paradox
One of the most counter-intuitive findings in sleep research: trying harder to fall asleep tends to make it harder, not easier.
British sleep researcher Colin Espie's 2006 paper in Sleep Medicine Reviews described what he called the attention–intention–effort pathway. When a person attends to sleep, intends to sleep, and exerts effort to sleep, the act of effort itself activates prefrontal and sympathetic systems that are incompatible with the state needed for sleep onset. Sleep is something the body falls into when nothing is in the way. Trying to do it interferes with letting it happen.
This model is the theoretical basis for paradoxical intention, the technique of trying not to fall asleep. Jansson-Fröjmark and colleagues' 2022 meta-analysis in Journal of Sleep Research reported some efficacy. The AASM 2021 guideline did not issue a recommendation on paradoxical intention — the panel concluded the evidence base wasn't sufficient to support a graded recommendation either way.
What the literature suggests practically:
- Clock-watching in bed is a documented amplifier of sleep effort.
- Performing relaxation techniques too deliberately can turn the technique itself into effort.
- Reframing wakeful time as resting time, rather than failing to sleep, has been associated with reduced arousal in some studies.
The sleep effort literature describes general patterns observed in clinical studies. Whether and how it applies to a specific situation is a question for a clinician.
The clinically validated playbook — what AASM 2021 describes
The 2021 AASM guideline (Edinger et al.) covers behavioral and psychological treatments for chronic insomnia in adults. The only Strong graded recommendation is multicomponent CBT-i. CBT-i is not a single technique — it is a package of components delivered by a trained clinician.
Stimulus control — Conditional
Originally described by Bootzin in 1972 as four components, expanded through the 1970s and 1980s into the five-component form widely cited today:
- Go to bed only when sleepy
- Use the bed only for sleep (and intimacy) — not for reading, phones, or TV
- If you can't fall asleep within roughly 20 minutes, leave the bedroom; return only when sleepy
- Maintain a consistent wake time, regardless of how the night went
- Avoid daytime naps (or limit them to short, early-day naps)
The AASM 2021 panel issued a Conditional recommendation for stimulus control as a stand-alone component. It is described as a core part of the multicomponent CBT-i package.
Sleep restriction therapy — Conditional
Originated in Spielman et al., 1987 in Sleep. The therapy compresses time in bed toward the actual amount of sleep being obtained, then expands it gradually as efficiency improves. Kyle et al.'s 2023 HABIT trial in *The Lancet* tested nurse-delivered sleep restriction in primary-care settings and reported sustained benefit at follow-up.
Safety note. The first weeks of sleep restriction tend to increase daytime sleepiness, which can affect driving and operation of machinery. The protocol is generally not applied to shift workers, people with untreated sleep apnea, or people with bipolar disorder. Clinical literature describes implementation under clinician supervision as standard practice.
Relaxation therapy — Conditional
Includes progressive muscle relaxation (PMR) and breathing techniques. Detailed in the next section.
Single-component cognitive therapy — no recommendation
Cognitive restructuring around sleep beliefs (for example, "if I don't get eight hours I'll fall apart tomorrow") was not given a graded recommendation as a stand-alone intervention by the panel — the evidence base was assessed as insufficient. As part of the integrated multicomponent CBT-i package, it is described as a core element.
Sleep hygiene alone — Conditional against
The guideline issued a Conditional recommendation against using sleep hygiene as a single-component treatment. It is described as having value only as one element among several within multicomponent CBT-i.
Where guidelines describe escalation
The American College of Physicians' 2016 clinical practice guideline (Qaseem et al., Annals of Internal Medicine) also describes CBT-i as the recommended first-line treatment for chronic insomnia in adults. Pharmacologic treatment is covered in a separate AASM guideline (Sateia et al., 2017) and is generally described as an option used after or alongside CBT-i, depending on availability and clinician judgment.
Routes to access CBT-i described in the literature include certified CBT-i clinicians (typically psychologists or sleep medicine specialists) and digital CBT-i programs delivered under clinician guidance.
Whether any specific component of CBT-i is appropriate for a given person — including whether sleep restriction can be safely undertaken — is a clinical decision made with a healthcare professional.
Conditional-grade tools — relaxation and brief therapies
The AASM 2021 panel issued Conditional recommendations for several stand-alone tools:
- Relaxation therapy. Progressive muscle relaxation traces back to Jacobson's 1929 work and involves deliberately tensing each major muscle group for several seconds and then releasing it. Donato and colleagues' 2026 meta-analysis in Journal of Psychosomatic Research pooled 31 randomized trials (n=2,277) and reported a sleep-quality standardized mean difference of −1.74 favoring PMR. Important caveat: heterogeneity across studies was very high (I²=92.1%), so the pooled effect should be interpreted cautiously rather than as a settled estimate.
- Brief therapies. Compressed multi-session interventions delivering the core elements of stimulus control and sleep restriction in primary-care-friendly formats.
Both are described in the literature as most effective when integrated into the broader multicomponent CBT-i package, rather than used in isolation.
Note. Paradoxical intention, biofeedback, intensive sleep retraining, and mindfulness-based therapies were assessed by the AASM 2021 panel as having insufficient evidence for a graded recommendation. Some have shown positive signals in individual studies — paradoxical intention in Jansson-Fröjmark 2022, for example — but the evidence base was not assessed as sufficient for guideline-level endorsement at the time of publication.
Popular techniques — what the evidence actually shows
This is the territory where internet content is the loudest. The mechanisms behind these techniques can be plausible, but the evidence base described in the literature is thinner than the marketing.
The military sleep method ("96% in 2 minutes")
- Origin: Lloyd "Bud" Winter's 1981 book Relax and Win: Championship Performance — a sports performance book, not a clinical text. The "96% in two minutes" figure is described in the book as a self-reported result from WWII U.S. Navy Pre-Flight School pilot training. There is no peer-reviewed clinical trial documenting this figure.
- Mechanism: Sequential muscle relaxation (face → shoulders → arms → legs) followed by visualization. Functionally a variant of progressive muscle relaxation with imagery.
- Honest read: No safety concerns. The relaxation mechanics are plausible. The "96% in two minutes" claim, however, is a book anecdote rather than clinical data. Trying it is fine; comparing yourself to that headline number is not.
4-7-8 breathing (Andrew Weil)
- Origin: A breathing pattern (4-second inhale, 7-second hold, 8-second exhale) popularized by integrative-medicine physician Andrew Weil.
- Evidence: No large randomized trial of 4-7-8 breathing with sleep latency or sleep efficiency as primary outcome has been published. It was not evaluated by the AASM 2021 guideline.
- Mechanism: Extended exhalation can increase parasympathetic tone via vagal pathways. Mechanism is plausible.
- Honest read: A low-risk technique. Calling it a "validated treatment" overstates the evidence; calling it a useful low-effort tool to try is fair.
Cognitive shuffle (SDIT, Beaudoin 2016)
- Origin: Luc Beaudoin (Simon Fraser University) and colleagues. The serial diverse imagining task (SDIT) involves mentally visualizing a sequence of unrelated, neutral words.
- Evidence: A single conference paper at SFU with roughly 154 participants reported reductions in pre-sleep cognitive arousal comparable to a structured problem-solving control. Not subsequently replicated in larger peer-reviewed trials.
- Honest read: A promising mechanism (intentional random imagery may bridge into the unintentional drift that characterizes sleep onset), but a single small study is not the same as a validated treatment.
What these three share: no documented harms; plausible mechanisms (mostly via PMR or vagal pathways); marketing claims that exceed the evidence. Research literature consistently describes them as supplementary tools rather than substitutes for the multicomponent CBT-i package described by the AASM 2021 guideline.
Environment and timing — what research describes
Even with every Tier 1 and Tier 2 technique applied, environmental and timing variables can dominate the result. The literature consistently describes these as the strongest single levers — often stronger than any specific behavioral trick.
Bedroom temperature
The Sleep Foundation describes approximately 65°F (18.3°C) as the commonly cited target, with the broader doctor-recommended range generally given as 65–68°F (15.6–20°C). The mechanism described in the literature involves the natural drop in core body temperature that begins about two hours before sleep onset; a cooler environment supports that cascade. Warm rooms have been associated with delayed sleep onset.
Light exposure timing
Chang and colleagues' 2015 PNAS study from Czeisler's lab compared four hours of evening reading on a light-emitting eReader to four hours of reading a print book under dim light. The eReader condition was associated with approximately 55% suppression of evening melatonin, a delay in dim-light melatonin onset of approximately 1.5 hours, and reduced next-morning alertness. Reducing screen brightness or screen exposure in the 30–60 minutes before bed is a frequently described practical implication.
Morning light exposure within 30 minutes of waking is described in circadian research as supporting cortisol normalization and aligning the next evening's melatonin onset.
Caffeine timing
Caffeine half-life is described in pharmacology references as averaging about 5 hours, with individual variation reported between 1.5 and 9.5 hours (Institute of Medicine, NCBI Bookshelf NBK223808). Gardiner and colleagues' 2024 randomized crossover trial in Sleep reported that 400 mg of caffeine taken 4 hours before bed extended sleep onset latency by an average of 14.2 minutes (p=.013) and latency to persistent sleep by 25.4 minutes (p<.001). At 100 mg taken 4 hours before bed, no statistically significant disruption was observed.
An afternoon caffeine cutoff (typically noon to early afternoon) is the most common practical implication described.
Pre-bed cognitive offloading
Scullin and colleagues' 2018 study in Journal of Experimental Psychology: General assigned 57 healthy young adults to write either a specific to-do list or a list of completed tasks during the five minutes before bed, with sleep onset measured by polysomnography. The to-do list group fell asleep on average about 9 minutes faster (15.8 minutes vs 25.1 minutes). The mechanism described is cognitive offloading — moving anticipated tasks from working memory onto paper reduces pre-sleep rumination.
Consistent schedule — what research describes as a strong correlate
Windred and colleagues' 2024 study in SLEEP, drawing on 60,977 UK Biobank participants, reported that sleep regularity predicted all-cause mortality more strongly than sleep duration. The most-regular quintile had 20–48% lower mortality than the least-regular quintile, depending on the adjustment model.
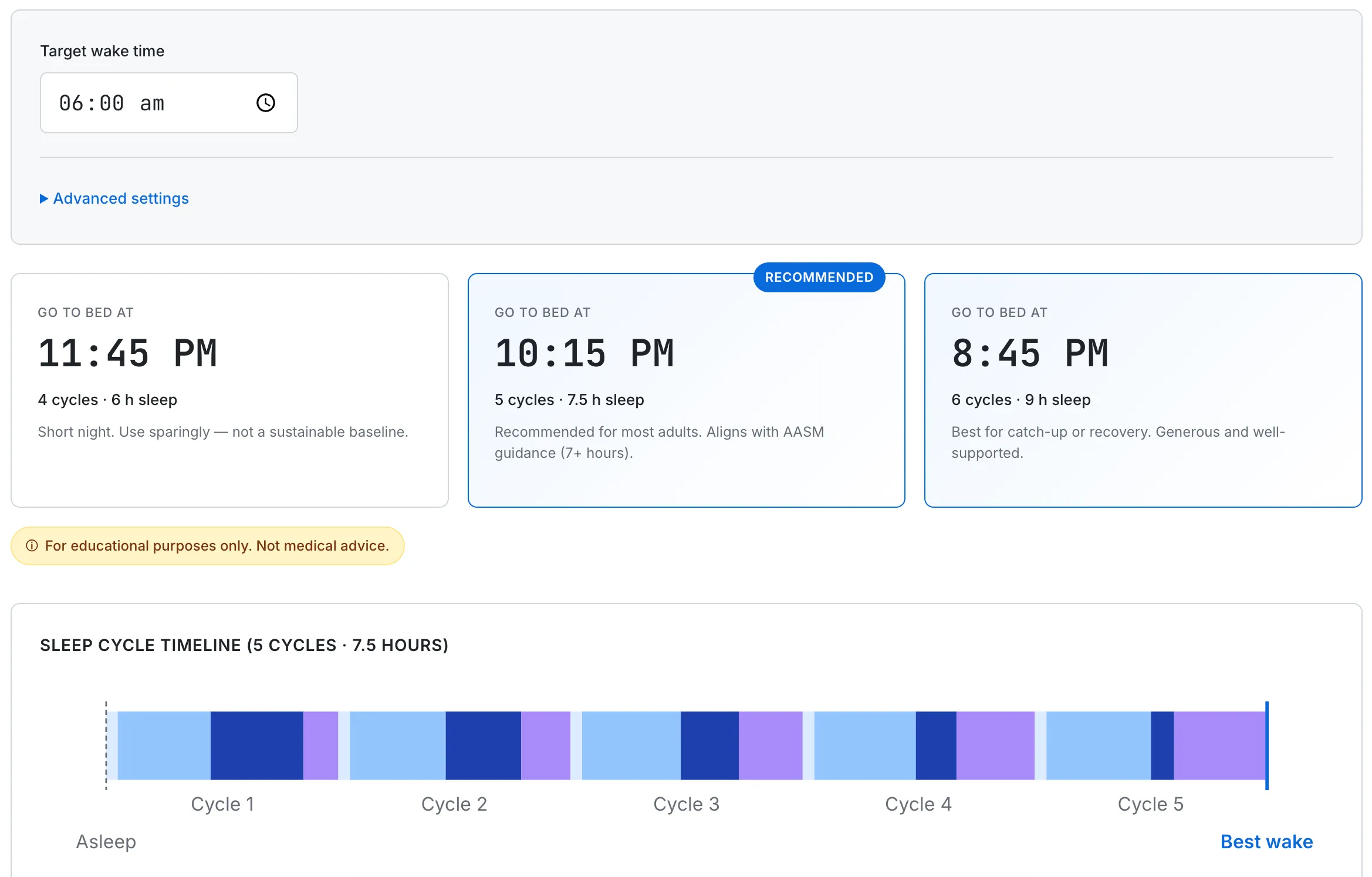
For sleep onset specifically, the same direction holds in the literature: a consistent bedtime trains the circadian system to anticipate sleep at that time. Research-based inference: a 7 a.m. wake time anchored every day is a stronger lever than any single in-bed technique. With a 90-minute cycle reference, 10:15 p.m. (5 cycles, 7.5 hours) or 8:45 p.m. (6 cycles, 9 hours) lands the alarm at the end of a cycle — the underlying mechanics are described in How Sleep Cycles Work, with cycle-aligned bedtimes for various wake times in What Time Should I Go to Bed if I Wake at 6 AM?.
Environment and timing recommendations describe general patterns from the research literature. Individual situations — including medications, chronic conditions, and shift work — can change how these apply, and discussion with a clinician is the typical next step.
Research consistently describes consistent schedule as one of the most reliable variables associated with faster sleep onset. The calculator finds the cycle-aligned window for whatever wake time you set.
When research describes escalation to a sleep specialist
Self-directed approaches have a documented limit. The DSM-5 criteria for chronic insomnia disorder describe the threshold at which clinical evaluation is generally recommended:
- Difficulty initiating sleep, maintaining sleep, or early morning awakening
- Occurring on at least three nights per week
- Persisting for at least three months
- Despite adequate opportunity to sleep
- Accompanied by daytime impairment (fatigue, attention, mood, or work / school effects)
When all five apply, the clinical literature describes evaluation by a primary-care clinician or sleep specialist as the appropriate next step.
Patterns described in clinical guidelines
- CBT-i is described as first-line in chronic insomnia by AASM 2021, ACP 2016, and several international guidelines. Pharmacotherapy is addressed in a separate AASM guideline (Sateia et al., 2017) and is generally described as a secondary option.
- Suspected physical causes — for example, when a partner reports loud snoring, witnessed breathing pauses, or limb movements — are typically evaluated separately (sleep study, blood work) before behavioral approaches alone are pursued.
- Early morning awakening combined with low mood persisting two or more weeks is described in clinical literature as a marker for which a depression evaluation is generally appropriate. (See Why Am I Tired After 8 Hours of Sleep? for a related diagnostic framing.)
The escalation criteria summarized here describe what clinical guidelines lay out. Whether a specific situation meets those criteria, and what the appropriate evaluation looks like, is determined by a clinician.
Frequently Asked Questions
How long should it take to fall asleep?
Normal sleep onset latency is generally described as 10–20 minutes. Falling asleep within five minutes is more often a sign of sleep deprivation than of being well-rested. Routinely needing more than 30 minutes, at least three nights a week for three months with daytime impairment, is the DSM-5 threshold at which clinical guidelines describe evaluation for chronic insomnia.
Does the military sleep method really work in 2 minutes?
The "96% in two minutes" figure comes from Lloyd "Bud" Winter's 1981 sports book Relax and Win, not from a clinical trial — no peer-reviewed study documents it. The technique itself is functionally a variant of progressive muscle relaxation with visualization, so it is low-risk and plausible to try. Comparing yourself to the headline number, however, is not realistic.
What is the most effective treatment for chronic insomnia?
Multicomponent cognitive behavioral therapy for insomnia (CBT-i) is the only treatment given a Strong recommendation in the AASM's 2021 behavioral treatment guideline, and the American College of Physicians' 2016 guideline also describes it as first-line. It is a package of components — stimulus control, sleep restriction, relaxation, and cognitive restructuring — typically delivered by a trained clinician rather than a single technique.
Does 4-7-8 breathing help you fall asleep?
No large randomized trial has tested 4-7-8 breathing with sleep latency or sleep efficiency as a primary outcome, and it was not evaluated in the AASM 2021 guideline. The extended exhale can plausibly increase parasympathetic tone via vagal pathways, so it is a low-risk, low-effort tool to try — but calling it a validated treatment overstates the evidence.
What bedroom temperature is best for falling asleep?
Approximately 65°F (18.3°C) is the commonly cited target, per the Sleep Foundation, with the broader doctor-recommended range generally given as 65–68°F. Core body temperature naturally begins dropping about two hours before sleep onset, and a cooler room supports that cascade — warm rooms have been associated with delayed sleep onset.
This article summarizes peer-reviewed research and clinical guidelines for informational purposes only. It is not medical advice, diagnosis, or treatment recommendation. Sleep restriction therapy and other clinical protocols described above carry safety considerations (for example, daytime sleepiness affecting driving) and are typically implemented under clinician supervision. If you have ongoing sleep difficulties, suspect a sleep disorder, or experience persistent fatigue, please consult a licensed healthcare professional. Information here represents the published literature as of April 2026 and may be revised as guidelines and evidence evolve.