How Much Sleep Do Children Need by Age? Newborns, Infants, Toddlers, and School-Age
The chart goes by age band — but what it doesn't show is that infant sleep is structurally different from adult sleep, that nap drops happen on a range rather than a date, and that "sleep regression" isn't actually a clinical diagnosis.
This is an informational summary of pediatric sleep guidelines (AAP, AASM, NSF, CDC) and peer-reviewed research. It is not medical advice, a diagnostic tool, or a sleep training guide. Children's sleep needs vary widely with individual development, temperament, and health — the age ranges and patterns described here are population averages, not targets every child must hit. For ongoing concerns about a child's breathing during sleep, persistent severe disruption, or sleep-related daytime behavior changes, the American Academy of Pediatrics describes consulting a pediatrician as the appropriate next step.
A friend texted me at 1 AM last week. Her four-month-old had been sleeping eight hours straight the previous week — and was now waking three times a night. "What did I do wrong?" The question of how much sleep do children need at any given age is the one parents reach for first, and the honest answer is that at four months the infant brain is in the middle of rebuilding its sleep architecture from the ground up — shifting from the newborn's two stages (active sleep and quiet sleep) toward the four-stage adult arrangement of N1, N2, N3, and REM. Infants spend roughly 50% of their sleep in REM — more than twice the adult share. Whether that maturation reliably produces the textbook "four-month sleep regression" is more debated than parenting media tends to suggest. The underlying biology — that infant sleep is a structurally different system, not just less sleep — is well documented.
The short answer. The AASM recommends, per 24 hours and including naps — 12–16 hours for infants 4–12 months, 11–14 hours for toddlers 1–2 years, 10–13 hours for preschoolers 3–5 years, and 9–12 hours for school-age 6–12 years. The AASM did not issue a formal recommendation for newborns 0–3 months because of the limited published outcomes at that age — the NSF and the CDC describe a typical range of about 14–17 hours per 24 hours, distributed across multiple naps. Naps are part of those totals — a one-year-old's "11–14 hours" is usually about 11 hours overnight plus two naps of roughly 90 minutes. Infant architecture genuinely differs from adult architecture: newborns spend roughly half their sleep in REM and enter REM directly at sleep onset, with adult-like stage proportions emerging gradually around age five.
This post walks through (1) the per-age chart with naps included, (2) why infant sleep is a different system rather than just less of the adult one, (3) how naps progress — how many, how long, and when each one drops, (4) what the literature actually shows about sleep regressions, and (5) the patterns pediatric sleep medicine describes as worth raising with a clinician.
How much sleep do children need by age — the full chart
The most cited single reference for U.S. pediatric sleep medicine is the 2016 AASM consensus statement (Paruthi et al.). An AASM expert panel reviewed 864 papers across eight health domains — attention, behavior, learning, cardiovascular, metabolic, mental health, immune function, and accidents — using the RAND Appropriateness Method. The methodology paper, Watson et al. 2016, describes the panel-and-vote process. The broader chart that places these pediatric numbers next to adult and older-adult ranges lives in How Many Hours of Sleep Do You Need by Age? — this post is the zoom-in on the pediatric portion.
The crucial framing — these are total hours per 24 hours, including naps. A common misreading is to treat "11–14 hours" as a target for overnight sleep alone. For a one-year-old, the 11–14 typically pencils out to about 11 hours overnight plus one to two hours of afternoon nap.
The AASM was explicit about why it issued no formal newborn recommendation. The 2016 paper states: "Recommendations for infants younger than 4 months are not included due to the wide range of normal variation in duration and patterns of sleep, and insufficient evidence for associations with health outcomes." That gap is filled by the CDC, which describes 14–17 hours as typical for newborns, and by the National Sleep Foundation, which describes 14–17 hours and notes that some newborns sleep up to 18 — typical-range descriptions, not outcome-validated recommendations.
| Age | Total sleep (incl. naps) | Naps per day | Typical nap length | Developmental note |
|---|---|---|---|---|
| 0–3 months (newborn) | 14–17 h (CDC); up to ~18 h described by NSF. No formal AASM recommendation. | 3–5+, irregular | 30 min – 4 h, variable | ~50% REM (active sleep); only two stages distinguishable; cycles 40–60 min; REM-onset |
| 4–12 months (infant) | 12–16 h (AASM / CDC) | 2–3 (third nap drops 6–9 mo) | ~1–1.5 h each | Maturation toward four stages; sleep spindles around 3 mo term-equivalent; nighttime consolidation around 10.5 h (Mindell 2016) |
| 1–2 years (toddler) | 11–14 h (AASM / CDC) | 1–2 (2→1 transition 14–18 mo) | 1–2 h afternoon nap | Sleep cycle lengthens toward ~90 min; daytime sleep declines |
| 3–5 years (preschooler) | 10–13 h (AASM / CDC) | 1 or 0 (final drop 3–5 yr) | ~1 h when napping | Stage proportions approach adult-like profile around age 5 |
| 6–12 years (school-age) | 9–12 h (AASM / CDC) | 0 (most stop by ~6) | n/a | Adult-like 90-minute cycle; insufficient sleep linked to attention, behavior, learning concerns |
Mindell's 2016 longitudinal data describes how infant sleep tends to consolidate between 3 and 7 months into roughly 10.5 hours overnight plus two naps of about 1.5 hours each. That is a useful translation when the chart's averages need to be turned into something that resembles a daily routine. The AAP's HealthyChildren page notes plainly that "sleep needs vary from one person to another" — a child whose pattern lands a little outside the band is not, by that fact alone, a problem.
Why infant sleep is a different system, not just less sleep
The finding that infant sleep is structurally different from adult sleep — not simply more of it — is well established in pediatric sleep medicine. Four features matter most.
REM share — about 50% in newborns versus about 20% in adults. A term newborn spends roughly half of total sleep in REM, sometimes called active sleep at this age (NSF). In preterm infants the proportion is higher still, in the 40–60% range, and in the most premature infants even higher proportions have been reported in some studies (2024 review). Adult REM sits around 20%, which means a newborn devotes more than twice as many hours to REM as an adult sleeping the same number of hours.
Sleep cycle length — 40–60 minutes in newborns versus about 90 minutes in adults. Newborn cycles are markedly shorter. The cycle gradually lengthens toward the adult ~90 minutes by around age five. The science of the adult 90-minute cycle is covered in detail in How Sleep Cycles Work; this post focuses on how the pediatric version differs.
REM-onset sleep — infants enter REM immediately at sleep onset. This is the most visible structural difference from adult sleep. Adults pass through N1 → N2 → N3 before reaching REM about 70–90 minutes in. Infants drop into active sleep (the REM equivalent) almost as soon as they fall asleep — which is why parents so often see a baby just drifting off and within a minute notice rapid eye movement, twitches, or smiles. The full progression of adult stages is mapped out in How Sleep Cycles Work.
Two stages, not four. Newborn EEG distinguishes only active sleep and quiet sleep (2024 review). The adult four-stage arrangement (N1, N2, N3, REM) emerges gradually — sleep spindles appear around three months term-equivalent, clearer slow-wave sleep stabilizes between five and eight months, and stage proportions approach the adult profile by around age five.
Why so much REM — Roffwarg's hypothesis. The 1966 ontogenetic hypothesis (Roffwarg) has remained a backbone framework in infant sleep research. The proposal is that the high-REM newborn period supports the structural maturation of sensory and motor cortex — providing endogenous activation that helps build thalamocortical connectivity in the absence of waking experience. The 2024 review notes that this remains the dominant framework in the field.
The implication is that frequent waking in infancy is less a "sleep problem" than a downstream consequence of the underlying biology. Cycles are short, REM share is high, and the end of a REM bout sits adjacent to a brief light-or-wake-adjacent window. Adults usually transition smoothly into the next cycle. Infants frequently surface fully — and that is what most caregivers experience as nighttime waking.
How many naps does a 1 year old need — and how naps drop with age
Nap progression is more variable than the chart's averages suggest. The framing pediatric guidance literature uses is that every transition is described as a range, not a fixed age. AAP-aligned guidance describes nap drops as child-driven rather than calendar-driven — a child consistently skipping a nap for one to two weeks is the cue, not the birthday.
Newborn (0–3 months). Three to five or more naps a day, anywhere from 30 minutes to four hours each. Mindell 2016 describes sleep sessions in this period as "primarily lasting less than 3.5 hours throughout the day." The day–night distinction is weak and circadian rhythm is not yet entrained.
4–6 months. Typically three naps a day, each 30–90 minutes (NSF). Nighttime sleep starts to lengthen and a recognizable consolidation pattern begins to appear.
7–12 months. Typically two naps a day, each 60–120 minutes. The pattern Mindell 2016 describes — about 10.5 hours overnight plus two naps of roughly 1.5 hours each — is the modal arrangement. The third nap usually drops between 6 and 9 months.
1–2 years. The 2-to-1 nap transition typically lands between 14 and 18 months, though some toddlers transition earlier or later. The settled arrangement is one afternoon nap of one to two hours. A short window of disruption is sometimes reported around the same age (see the next section).
3–5 years. One nap or none. The NSF reports that most children stop regularly napping by around age 4, with about 30% still napping at 5 and roughly 10% at 6. The final drop spans 3–5 years — a five-year-old who still naps is well within the typical band.
6–12 years. The NSF notes that "although many children stop napping by age 6," habitual napping persists in some children. Past school age, regular napping more often reflects insufficient overnight sleep than a developmental need for daytime sleep.
One reframing — these numbers are population averages. A child whose transition lands several months on either side of the median is not, by that fact alone, off-pattern. Caregivers running on broken sleep through any of these transitions can find the eleven causes of adult fatigue and a four-week self-check covered in Why Am I Tired After 8 Hours of Sleep?.
Infant sleep regression — what the literature actually shows
"Sleep regression" has become near-universal in parenting media — typically described as occurring at 4 months, 8–10 months, 12 months, 18 months, and 2 years. The shorthand definition is a temporary period (usually 2–6 weeks) of disrupted sleep — increased night waking, shorter naps, bedtime resistance — in a previously settled infant or toddler. How that label is treated in peer-reviewed pediatric literature is more nuanced than the parenting framing suggests.
The research-base caveat. Peer-reviewed pediatric sleep medicine tends to use terms like "sleep maturation" or "sleep fragmentation." Sleep regression is a parenting term, not an academic one. There is no formal entry for sleep regression in DSM or ICSD-3 (the International Classification of Sleep Disorders). The label captures a real lived experience for many caregivers — but the underlying mechanism is not as cleanly discrete as the timeline implies.
4-month regression. The mechanism most often cited is the two-stage to four-stage transition described above. The NSF page on the 4-month regression describes "rapid brain and nervous system development" producing "instability in sleep."
An honest caveat — an objective dip at four months is not consistently observed. Emily Oster's ParentData synthesis reviewed three lines of evidence — Mindell 2016's iPhone-app longitudinal data, a 2018 review, and a 60-person longitudinal study — and concluded that a consistent objective sleep dip at the four-month mark does not appear cleanly in measurement data. Parent reports and wearable or longitudinal recordings do not always converge. The strong felt experience that disruption clusters at four months is real for many families. Whether it represents a universal neurological event every infant must pass through is less well supported by the available measurement evidence.
One important Mindell finding. Longitudinal data suggest that night-waking frequency does not follow a simple linear decrease across the first year, with some studies showing wakings remaining stable or rising slightly in the second half of infancy. The pattern is not a smooth descent — disruption is distributed across maturation rather than concentrated at any single age.
8–10 months. Separation anxiety onset, motor milestones (crawling, pulling up), and cognitive leaps tend to overlap in this window. The literature framing is generally that the disruption reflects multiple contributors rather than a single mechanism.
18 months. The NSF describes the 18-month period as one of the more frequently reported windows of disruption, often associated with the transition from two naps to one and emerging language and autonomy. The same NSF page also includes a candid caveat: "Many toddlers do not experience a sleep regression at 18 months. Sleep patterns unfold differently for every child." Even the source most commonly cited for the 18-month label declines to claim universality.
Taken together — sleep regressions describe a phenomenon that some children experience at some times. They are not as universal, nor as clocked to specific ages, as the parenting framing implies. The label can be a useful shorthand without being a diagnosis.
When pediatric sleep medicine describes raising a concern with a clinician
This section is not a diagnostic tool. The patterns below are described in pediatric sleep medicine as starting points for a clinical conversation — not as a self-administered checklist.
The AAP 2012 OSA Clinical Practice Guideline. The AAP 2012 guideline on Diagnosis and Management of Childhood Obstructive Sleep Apnea is the standard U.S. reference for pediatric OSA. A core recommendation is that all children and adolescents be screened for snoring at well-child visits. The guideline describes signs that warrant clinical evaluation, including frequent loud snoring (multiple nights per week), witnessed breathing pauses, gasping or restless sleep, frequent awakenings, mouth breathing, and daytime symptoms such as behavior or learning concerns. The full AAP guideline is paywalled and the precise composite criteria are described in detail there — what's worth taking from this summary is the framing: not every loud breathing night is concerning, and the patterns the guideline describes are about persistence, accompanying symptoms, and daytime impact, not single-night observations.
The diagnostic standard — pediatric polysomnography. Adult OSA screening commonly uses questionnaires like STOP-BANG, which is a different framework that does not transfer to children. Pediatric OSA follows its own clinical pathway, with pediatric polysomnography (in-lab sleep study) as the diagnostic standard. The adult use of STOP-BANG is summarized in Why Am I Tired After 8 Hours of Sleep? — to be clear, that adult tool is not what pediatric clinicians use, and the pediatric pathway is governed by separate guidelines.
When a regression-like period stretches longer than expected. Typical sleep regression windows are described as 2–6 weeks. When disruption persists well beyond that range and is accompanied by significant daytime effects — behavioral changes, learning difficulties, persistent mood changes — pediatric sleep medicine literature describes that as a reasonable inflection point for a clinical conversation rather than continued watchful waiting.
Insufficient sleep and functional outcomes. The AASM/Paruthi 2016 statement summarizes evidence that chronic insufficient sleep in children is associated with attention, behavior, and learning problems. That is not a prescription — it's a framework for noticing when persistent sleep disruption may not be a passing phase.
Variability is normal. The AAP's HealthyChildren page is direct that "sleep needs vary from one person to another." A child whose pattern differs from the chart's median is not, on that basis alone, a flag. What pediatric literature describes as a flag is persistent disruption combined with measurable daytime impact — that combination is the signal, not absolute hours by themselves.
Caregivers running on chronically broken sleep can find a cycle-aligned bedtime — for a 6 AM alarm, a 10:15 PM bedtime that lands the alarm at the end of a cycle is an example — useful when the goal is to rebuild adult recovery quality between night wakings, not to add hours that the household schedule cannot give.
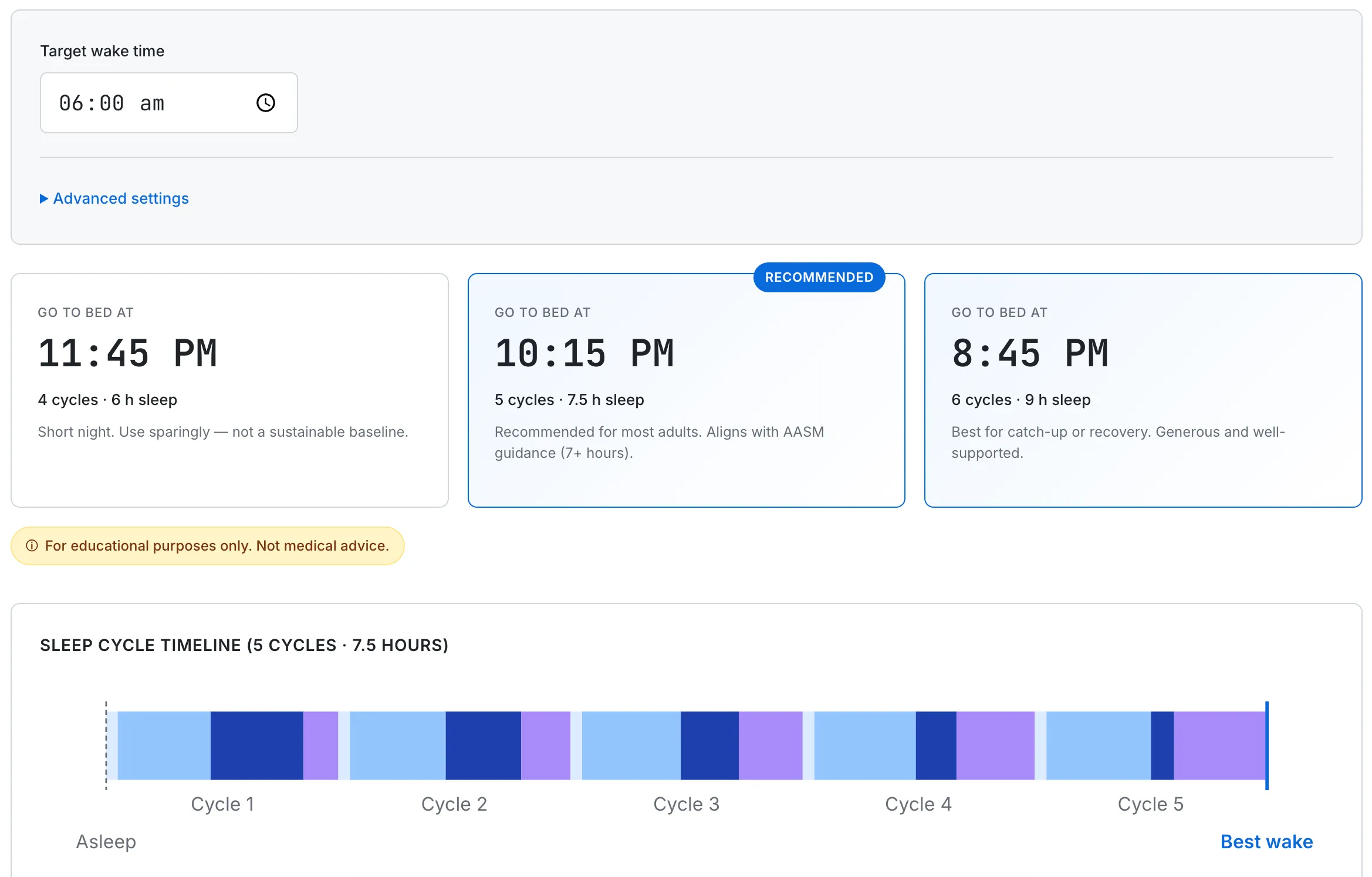
For caregivers managing their own sleep around a child's schedule, the calculator shows cycle-aligned bedtimes — 5 cycles (7.5 hours) or 6 cycles (9 hours) — so the alarm lands at the end of a cycle rather than mid-cycle.
This guide summarizes general pediatric sleep medicine drawn from peer-reviewed sources and consensus statements (AAP, AASM, NSF, CDC), and is for educational use only. Individual children's sleep needs vary considerably — the descriptions here are population averages, not targets. None of this is medical advice, sleep training advice, behavioral protocol, or a substitute for clinical evaluation. For persistent sleep difficulties, concerns about breathing during sleep, or significant daytime behavioral changes, professional pediatric sleep guidelines describe consulting a pediatrician or pediatric sleep specialist as the appropriate path. This summary reflects published literature current to April 2026 and will be updated as guidelines and evidence evolve.